KEY POINTS
Abdominal and thoracic injuries should be considered as one complex—torso trauma.
Prioritization of intervention in torso trauma is based on the relative threat to life from specific injuries.
In managing torso trauma, the surgeon must be prepared to explore the chest and/or abdomen because the source of instability frequently is not obvious.
The major decision in assessing the traumatized abdomen is to recognize the need for surgical exploration.
In general, indications for surgical intervention in abdominal trauma are perforation, penetration, and hemorrhage.
An organ-specific diagnosis is not necessary to establish the need for laparotomy in trauma.
Ultrasound, peritoneal lavage, and computed tomographic (CT) scan are important tools in assessing the traumatized abdomen when physical examination alone is unreliable.
Most thoracic injuries can be managed appropriately by simple measures aimed at correcting thoracic sources of hypoperfusion and hypoxemia.
Emergency thoracotomy should be considered in the unstable or unresponsive patient when this technique could potentially reverse the source of instability.
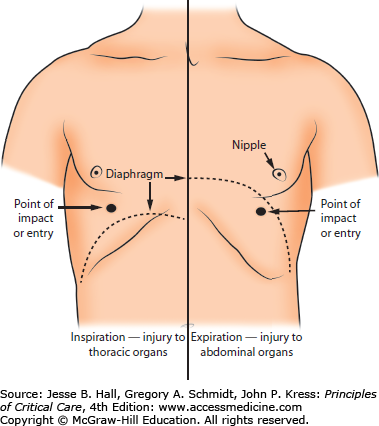
Injuries involving the chest and abdomen may be considered as a single complex—torso trauma. This strategy is based on several factors. The configuration of the diaphragm and its attachment to the rib cage result in marked variability in its position with respiration and thus in demarcation of the thoracic and abdominal cavities. It is not unusual for the diaphragm to traverse distances of over 15 cm between the inspiratory and expiratory phases of respiration. The diaphragm may be at the level of the nipple line during full expiration and well below the costal margin during full inspiration, with corresponding shifts of the abdominal and thoracic contents (Fig. 120-1). This phenomenon, together with the variable trajectory of objects or forces after penetrating the torso, makes it virtually impossible in many instances to determine on the basis of the external point of impact or penetration whether intrathoracic or intra-abdominal injury has been sustained. The concept of torso trauma ensures that injuries in one cavity will not be overlooked while injuries in the other are being managed.
The initial approach in trauma management is to secure the airway, to maintain respiration, and to identify and control hemorrhage and institute immediate fluid resuscitation as required. Definitive management of intra-abdominal or thoracic injury may be necessary as part of this resuscitative phase, particularly if the source of instability is major hemorrhage in the thoracic or abdominal cavity. Although it may be possible to identify a specific source in the thorax or abdomen for the abnormal hemodynamics in the trauma patient, it is frequently impossible to be absolutely certain of such a source. Therefore, a decision has to be made to approach the hemodynamically abnormal patient through either a laparotomy or a thoracotomy if a source outside the thorax or abdomen has been ruled out. With this approach, one must be prepared to stop exploration of one cavity when it becomes obvious that the source of the hemodynamic abnormality is in the other.
CLASSIFICATION OF TORSO TRAUMA
Generally, torso trauma may be classified into two broad groups: penetrating and blunt. As indicated earlier, any penetrating missile entering inferior to the nipple line can produce diaphragmatic, intrathoracic, or abdominal injuries. Similarly, blunt injuries may disrupt intrathoracic contents as well as intra-abdominal contents either directly or indirectly through fractures of the lower ribs, which then puncture intra-abdominal organs such as the spleen, liver, and stomach.
A more clinically applicable method of classifying torso trauma involves two categories. The first category consists of injuries that are immediately life threatening and thus require immediate intervention because of cardiorespiratory or hemodynamic compromise. The other category includes injuries in a relatively hemodynamically normal patient. These latter injuries are considered to be potentially life threatening because, if left unattended, they eventually may threaten the patient’s survival.
Occasionally, neck injuries, particularly the penetrating type, may involve intrathoracic structures. In addition to causing vascular injury (which may present with hemorrhage or ischemic sequelae), injury to the thoracic duct (resulting in chylothorax), violation of the pleura (resulting in pneumothorax), or penetrating neck wounds may affect any of the intrathoracic structures, depending on the pathway of the offending weapon.
The neck traditionally is divided into three anatomic regions for the purposes of categorizing penetrating wounds. Zone I extends from the cricoid to the clavicle, zone II from the cricoid to the angle of the mandible, and zone III lies between the angle of the mandible and the base of the skull.
Penetrating wounds of the neck should be explored in the operating room under sterile conditions with adequate anesthetic support. A preoperative plain x-ray of the neck if the patient is stable could provide information such as depth of penetration and the presence of air in the tissues, hematoma, airway deviation, etc. Impaling objects should be removed only in the operating room with vascular equipment available and a securely controlled airway in place. Although there is reasonably good agreement that zone III injuries should be investigated with angiography, the use of angiography and other diagnostic modalities in zone II injuries is controversial because this area can be assessed thoroughly and more easily through direct surgical exploration in the operating room. Diagnostic modalities include angiography, endoscopy, contrast radiography, and computed tomography (CT).
A nasogastric tube should be inserted in the operating room, preferably after the airway is securely controlled by endotracheal intubation, because retching during the insertion of such a tube could lead to clot dislodgment, hemorrhage, and airway compromise. The possibility of intrathoracic injury should always be considered in patients with penetrating neck wounds. The chest therefore should be prepared and draped adequately in the event that thoracic exploration is necessary for repair of intrathoracic injury or possible vascular control for vascular injuries in the neck.
THORACIC INJURIES REQUIRING IMMEDIATE INTERVENTION
Although thoracic injury frequently is associated with trauma-related deaths, less than 10% of blunt chest injuries and only 15% to 30% of penetrating chest injuries require open thoracotomy. Lifesaving skills for dealing with thoracic trauma generally are within the scope of most practicing intensivists. Of the injuries that require open surgical intervention, most do not require the expertise of a trained thoracic surgeon. From the intensivist’s standpoint, resuscitative measures are aimed at correcting hypoxemia and maintaining normal hemodynamic status. These two aims are achieved by techniques for establishing patency of the airway, chest decompression for evacuating fluid or air, pericardiocentesis, and vascular access for fluid administration.
In addition to upper airway obstruction, the following thoracic injuries require immediate intervention:
Tension pneumothorax
Open pneumothorax
Cardiac tamponade
Massive hemothorax
Massive pneumothorax
Traumatic air embolism
Flail chest
Since all of these conditions require immediate intervention, the intensivist who sees such patients must be prepared to institute therapy before any other physician is available. To guide appropriate intervention, a brief description of the pathophysiology, diagnosis, and treatment principles for each of these conditions follows. In all cases, the airway must be secured and adequate intravenous (IV) access established.
This occurs when a one-way valve mechanism exists after chest wall or lung injury. Gas enters the pleural space but has no escape, and with each subsequent respiratory cycle, there is increased intrapleural pressure. This increased tension causes the ipsilateral lung to be compressed and displaced to the opposite side. With the resulting mediastinal shift, there is not only compromise of ventilation and gas exchange from the ipsilateral collapsed lung but also kinking of the major veins at the thoracic inlet of the neck and at the diaphragmatic entrance of the inferior vena cava, thus compromising venous return to the heart. Continued shift of the mediastinum eventually compresses the contralateral lung as well, producing further ventilatory compromise. This combination of hypoperfusion and hypoxemia can be lethal, and immediate treatment is required. The diagnosis is suspected in a patient who presents with chest trauma, tachypnea, severe dyspnea, jugular venous distention, decreased air entry, and hyperresonance on the affected side and, sometimes, a clinically detectable shift of the trachea to the opposite side with hypotension.
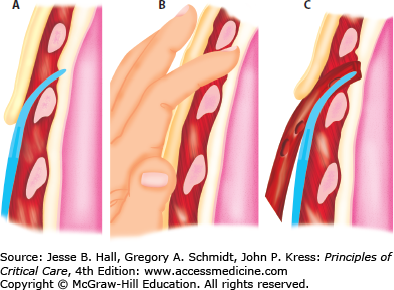
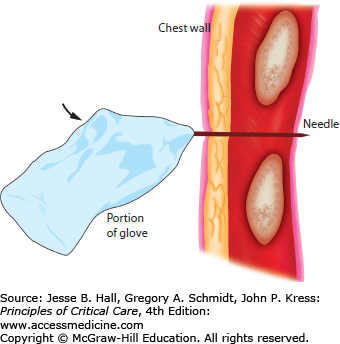
The treatment is immediate decompression of the pleural space, which is accomplished initially by inserting a large-bore needle into the pleural space at the second intercostal space in the midclavicular line or the fourth to fifth intercostal space just anterior to the midaxillary line. If a plunger syringe is used with the needle, an immediate spontaneous rise of the plunger in the barrel will be seen. This procedure should be followed by formal insertion of a chest tube. Briefly, the technique of chest tube insertion requires an incision down to the pleura in the fourth to fifth intercostal space just anterior to the midaxillary line. The large-bore chest tube (F32-F36) is inserted directly with a clamp after verification by finger palpation that the pleural space has been entered and there are no pleural adhesions (Fig. 120-2). When needle decompression is performed and the chest tube is not immediately available, the needle may be inserted through the finger portion of a glove so that air may exit but not enter the pleural space from the atmosphere (Fig. 120-3). Once the chest tube is inserted, it is connected to an underwater seal system with the option of applying suction.
FIGURE 120-2
Technique of chest tube insertion. The incision is made 2 cm below the chosen interspace, and the clamp (A) followed by the finger (B) is inserted into the pleural space above the upper border of the rib. The tube is inserted and directed with the Kelly clamp (C). The tube is then gently directed posteriorly and toward the apex.
In many trauma centers, immediate availability of the chest tube and suction device allows chest tube decompression without prior needle decompression in experienced hands.
In open pneumothorax, there is free communication through a chest wall wound between the pleural space and the atmosphere. Entry of air with each respiratory cycle results in progressive collapse of the ipsilateral lung. The larger the defect in the chest wall, the greater is the rate at which pleural air accumulates, and the more rapid is the collapse of the ipsilateral lung. This pathophysiology is similar to that in tension pneumothorax because collapse of the lung and shift of the mediastinum to the opposite side will cause hypoxemia and decreased venous return. During spontaneous breathing, the inability to generate negative intrapleural pressure on the affected side results in progressive lung collapse on this side. The diagnosis usually is obvious, with a visible open wound in the chest wall and a characteristic loud noise created from atmospheric air entry into the pleural space.
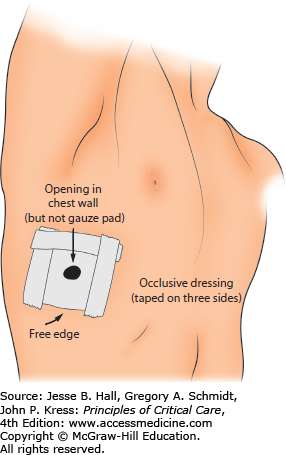
The first principle in treating this injury is occlusion of the open wound. This usually can be accomplished with an occlusive gauze dressing (Fig. 120-4). Larger defects will require much larger dressings, and major defects that cannot be occluded readily by dressing technique will require support of the patient with endotracheal intubation and positive-pressure ventilation until formal surgical repair of the chest wall defect can be accomplished in the operating room. Positive pressure ventilation allows the expansion of the lung without the need for generating negative intrapleural pressure as occurs during spontaneous unassisted breathing. After the opening in the chest wall is occluded, a chest tube should be inserted through a separate opening, as indicated earlier. Figure 120-4 shows a technique whereby a temporary occlusive dressing can be applied that allows decompression of the pleural space as well as occlusion of the opening. The nonpermeable dressing is applied over the opening and secured on all but one side. This allows egress of air from the pleural space but prevents air from entering the pleural space.
Cardiac tamponade occurs when fluid accumulation in the pericardial sac interferes with cardiac filling. Elevated pericardial pressure decreases transmural filling pressures of the cardiac chambers, resulting in diminished filling and stroke volume of the right and the left side of the heart. Cardiac output falls, with an attendant decrease in systolic blood pressure and pulse pressure.
The diagnosis of cardiac tamponade is one that requires a high index of suspicion and should be considered in any patient who has blunt or penetrating trauma to the chest and is hypotensive without any obvious signs of blood loss. The classic triad described by Beck of hypotension, elevated venous pressure, and muffled heart tones is not always present or easily discernible. The status of the neck veins is particularly important in distinguishing hypotension caused by hypovolemia from that caused by cardiac tamponade. In the former case, the neck veins are flat, whereas in the latter, they are distended. If hypovolemia coexists with cardiac tamponade, neck vein distention may not be discernable. Also a struggling or straining patient may produce misleading bulging of the neck veins, which must be taken into consideration. An increase in pulsus paradoxus (the difference in systolic blood pressure between inspiration and expiration) above 10 mm Hg suggests the diagnosis of cardiac tamponade. However, in the emergency setting it may be difficult to quantitate the degree of pulsus paradoxus. During arterial pressure transduction in the ICU, it is possible to measure pulsus paradoxus accurately. The physician should note the difference between systolic blood pressure during inspiration and expiration. The pressure waveform will exhibit a lower peak level in inspiration, with higher peak levels in expiration. The difference between the two peaks is the measure of the degree of pulsus paradoxus. The degree of pulsus paradoxus may be determined at the bedside by listening for the first set of sounds with the sphygmomanometer slowly deflating. The first set of sounds represents the systolic blood pressure on expiration. As the pressure in the cuff is slowly released, the gaps in systolic blood pressure sounds between inspiration and expiration disappear, and there is an increased frequency of sounds heard with the stethoscope. The difference between the initial pressure and the pressure when the gaps in sounds have disappeared is the degree of pulsus paradoxus. Since distended neck veins and hypotension are present in both tension pneumothorax and cardiac tamponade, differentiation between these two conditions is important but at times difficult. The physician must rely on evidence of hyperresonance and decreased breath sounds that will suggest tension pneumothorax. If a search for these signs still leaves doubt, the patient should be treated first for possible tension pneumothorax by insertion of a needle in the pleural space. This step can be performed quickly and will give the diagnosis as well as be therapeutic for a tension pneumothorax. Once tension pneumothorax is ruled out, one should proceed to treatment for cardiac tamponade if signs of circulatory compromise persist. If immediately available in the emergency setting, epigastric placement of an ultrasound probe is also helpful in diagnosing hemopericardium. In many trauma centers, ultrasound technology is immediately available in the ER and allows immediate identification of hemopericardium. The presence of hypotension, distended neck veins, and hemopericardium confirms the diagnosis of cardiac tamponade.
Although performance of a subxiphoid pericardial window in the relatively stable patient is acceptable, the initial treatment of cardiac tamponade consists of prompt pericardiocentesis. Many surgeons will resort to rapid thoracotomy rather than pericardiocentesis when cardiac tamponade is identified. Nonsurgeons skilled in pericardiocentesis will utilize this technique as a temporizing measure until thoracotomy is possible. If pericardiocentesis is performed, a 16- to 18-gauge needle that is at least 6 in long is used. It incorporates a catheter, and is attached to a 50-mm empty syringe with a three-way stopcock. If time permits, the skin below the xiphoid process is anesthetized, and an electrocardiographic lead is attached to the hub of the needle as the needle is inserted below the skin at roughly a 45° angle and advanced cephalad toward the tip of the left scapula. Gentle aspiration is maintained as the needle is advanced. A sense of “give” may be noted as the needle enters the pericardial sac. Nonclotting blood aspirated at this time confirms a pericardial position of the needle. If the needle is advanced into the myocardium, an injury pattern is seen on the electrocardiogram (ECG) monitor. If this is noted, the needle should be withdrawn slightly and then aspirated coincident with return to the previous baseline ECG tracing. Other ECG patterns, including premature ventricular contractions, may occur when the needle contacts the myocardium.
Although the pericardial sac can accommodate large volumes of fluid in chronic pericardial effusion without cardiac compromise, in acute pericardial tamponade, a volume as small as 100 mL can compromise cardiac function significantly. Similarly, withdrawal of as little as 20 to 50 mL of blood from the pericardial sac results in significant improvement in hemodynamic status. Apart from the signs noted earlier that suggest successful aspiration of the pericardial sac, recovery of blood that immediately clots in the syringe, particularly if the patient’s hemodynamic status does not improve, should raise the concern that the needle has penetrated the heart and that intracardiac rather than pericardial blood is being aspirated. As pericardiocentesis is being conducted, the operating room (OR) should be prepared; whether pericardiocentesis fails or succeeds and results in stabilization of the hemodynamic status, it should be followed by formal thoracotomy and repair of the lacerated heart. This usually is conducted through an anterolateral thoracotomy incision in the fifth intercostal space. However, a median sternotomy is an alternate route for anterior penetrating wounds. When the thoracic cavity is entered, the pericardium is identified, and a longitudinal incision is made in it, care being taken to avoid transection of the phrenic nerve. Blood is aspirated, and the laceration in the heart is identified and controlled quickly by digital pressure. With finger control of the bleeding point, interrupted sutures are placed and maybe secured with Teflon pledgets to repair the laceration. The pericardium may be then resutured, with a small opening (approximately 1 cm) left to prevent reaccumulation of blood in the pericardial sac. Other reported techniques for repair of the cardiac laceration include temporary Foley catheter insertion into the cardiac wound, followed by inflation of the balloon of the catheter and repair of the laceration. Skin staples also may be used to close the cardiac wound. In very rare circumstances, the laceration involves the coronary arteries. Formal repair of the artery will require heart-lung bypass and may be accomplished in the acute setting if the resources are immediately available. If the patient’s condition stabilizes and the bleeding and laceration have been controlled, then definitive therapy for the coronary artery laceration may be pursued subsequently on a semielective basis. In placing sutures for the cardiac repair, care should be taken to avoid incorporating and ligating coronary arteries.
Although most patients with traumatic hemothorax are relatively stable and do not require immediate surgical intervention, a few present with massive intrathoracic hemorrhage. This condition requires prompt diagnosis and immediate treatment to ensure survival. The mechanism of injury may be blunt or penetrating and generally involves disruption of a major central vascular structure or laceration of a systemic artery such as an intercostal artery or internal mammary artery. Intrathoracic hemorrhage usually arises from parenchymal lesions of the lung and stops spontaneously, particularly with reexpansion of the lung. The patient with massive intrathoracic hemorrhage presents initially with severe hypotension from blood loss and later with hypoxemia from collapse of the lung caused by the mass effect of the blood in the involved thoracic cavity. Apart from severe hypotension and tachycardia, these patients demonstrate dullness to percussion and decreased air entry on the involved side and a shift of the mediastinum to the opposite side. The central venous pressure or jugular venous pressure is usually low, but it may be elevated in the unusual circumstance that a mass effect from the blood contained in the thorax produces a mechanical obstruction to venous inflow into the chest.
The diagnosis is confirmed and treatment instituted by insertion of a large-bore chest tube, through which a large volume (frequently close to 2000 mL) of blood drains immediately, to be followed by a continuous drainage of blood at rates approximating 100 mL/h. If either of these conditions is present, the patient is considered to have a massive hemothorax requiring surgical intervention. These should not be considered absolute indications for thoracotomy but merely guidelines. The most important indicator of whether or not surgical intervention is necessary is whether the patient’s hemodynamics improve significantly and remain so after chest decompression and with fluid resuscitation. If bleeding continues at a rapid rate, or if the patient’s hemodynamic status cannot be normalized with rapid infusions of blood and crystalloid, surgical intervention is warranted. The involved chest is opened through a posterolateral incision. Once the blood has been evacuated from the pleural space, a search is made for the bleeding point. It is frequently necessary to clamp the hilum of the lung temporarily and to release it intermittently in order to identify the area of bleeding, which is repaired by direct suture. Occasionally, massive hemorrhage necessitates resection of the involved lung, which should be accomplished quickly using staple devices. Very occasionally, the bleeding is from a ruptured thoracic aorta. Usually patients with free bleeding into the thoracic cavity from a ruptured aorta exsanguinate at the scene or immediately thereafter. However, in certain instances, it is possible to salvage some of these patients by clamping the aorta proximal and distal to the laceration and expeditiously repairing the laceration or inserting an aortic graft prosthesis. If available, a preheparinized shunt may be used in these circumstances to bypass the lacerated area of the aorta and maintain perfusion of the distal aorta and spinal cord while the repair is undertaken. Occasionally, access to the bleeding source will require extension of the unilateral thoracotomy incision into the opposite chest by transection of the sternum (clam shell incision). Ligation of the internal mammary arteries will be necessary once the circulation is restored.
THE MASSIVELY BLEEDING PATIENT
As indicated previously, it is not always possible to determine precisely whether massive bleeding arises from a thoracic or an abdominal source. Therefore, it is crucial that the entire abdomen and chest be prepared and draped for exposure in the OR. In these circumstances, if the bleeding is into the right chest and the apparent site of impact or penetrating injury is in the lower right chest below the nipple line, laparotomy through an upper midline incision should be conducted because the source of the hemorrhage is usually a liver injury with penetration of the right hemidiaphragm. Where ultrasound assessment is immediately available, this may allow more precise location of the source of the hemorrhage and thus guide the location of the incision in the abdomen or thorax. Failure to reveal an abdominal source of hemorrhage at laparotomy will necessitate an anterolateral thoracotomy on the right side, which usually will reveal lacerated intercostal arteries, which should be identified and ligated. As indicated earlier, injuries to the low-pressure pulmonary vasculature usually are not associated with massive hemorrhage, and the bleeding stops spontaneously, particularly with reexpansion of the lung and decompression of the pleural space. If the impact is to the right upper chest or to any portion of the left chest, then massive hemorrhage should be treated by anterolateral thoracotomy on the bleeding side, and the incision should be extended as necessary to obtain control of the bleeding site. Occasionally, bleeding into the chest arises from a penetrating injury to the base of the neck. In these circumstances, the chest should be opened through a median sternotomy, with the option of extending laterally into the chest as well as above the clavicle to convert the incision to a trapdoor type of exposure. The median sternotomy under these circumstances allows better exposure of the vascular structures of the base of the neck than would be available through an anterolateral thoracotomy.1
Most patients with traumatic pneumothoraces present with signs characteristic of a pneumothorax but without any major degree of hemodynamic compromise, and the pneumothorax responds very promptly to chest tube insertion. Occasionally, however, the pneumothorax persists despite adequately functioning large-bore chest tubes and is accompanied by massive subcutaneous emphysema and continued hypoxemia and respiratory instability. The patient usually also has some degree of hemoptysis, which may be evidenced by blood draining through the endotracheal tube if the patient has been intubated, as is often the case. This scenario suggests the presence of a large tracheobronchial laceration and requires immediate surgical intervention.
The patient is placed immediately on 100% oxygen. If time allows, bronchoscopy should be performed to identify the level of the lacerated bronchial tree. However, thoracotomy is warranted even if the lesion is not identified or there is insufficient time to perform bronchoscopy. It is essential that one be certain that the chest tubes are functioning adequately in these circumstances, and if mechanical problems are ruled out, the patient should be taken to the OR promptly. Occasionally, for a right-sided bronchial leak, insertion of a balloon-tipped catheter down the right mainstem bronchus may allow ventilation of the normal left lung after the right bronchus is occluded by inflation of the balloon. This measure temporarily stabilizes the patient by decreasing the air leak on the involved side. It is technically very difficult to accomplish, however, and should not take priority over getting the patient to the operating room as quickly as possible. For a left-sided bronchial tear, the endotracheal tube may be directed into the right mainstem bronchus and the cuff of the endotracheal tube inflated. This would allow ventilation of the right lung until the left lung lesion has been repaired. In the OR, a double-lumen tube, if available, will allow selective ventilation of the normal lung. At surgery, the lesion is identified and repaired directly. If there is massive destruction of the bronchus with failure to achieve an anastomosis or a high risk of subsequent stenosis, lung resection should be considered. Successful thoracoscopic approaches for persistent air leak have also been reported.
The exact incidence of this entity in patients with multiple injuries is not known. However, to make the diagnosis, a very high index of suspicion must be maintained, and this diagnosis should be suspected in any patient with sudden cardiovascular collapse who demonstrates a neurologic deficit after chest injury, especially if these signs occur with the initiation of positive-pressure ventilation. In most cases, the diagnosis of traumatic air embolism is made at thoracotomy that is conducted on the basis of sudden collapse of a patient who has sustained major chest trauma. Occasionally, these patients may be quite stable initially, only to develop a focal neurologic deficit suddenly with cardiovascular collapse immediately after being placed on positive-pressure ventilation. Another sign suggestive of the diagnosis is the presence of bubbles within arterial blood drawn by arterial puncture, usually for blood gas analysis. It must be recognized, however, that the most common cause of air bubbles in the syringe is a loosely fitting syringe connector; this must be ruled out prior to making the diagnosis. Occasionally, air may be seen in the retinal arteries on funduscopic examination as well.
An anterolateral thoracotomy should be performed on the side of the penetrating injury or on the left side if no penetration is apparent. On entry into the thoracic cavity, prevention of further embolization is accomplished by cross-clamping the pulmonary hilum. An 18-gauge needle should be used for venting the most anterior surfaces of the left atrium, left ventricle, and ascending aorta. This maneuver is followed by compressing the root of the aorta between the thumb and index finger, which are placed in the transverse sinus. Massaging the heart should drive air bubbles out of the coronary microvasculature. Maintenance of a high systemic blood pressure, with α agonists if necessary, should help to force trapped air from the heart and brain through the microvasculature into the venous circulation. With reestablishment of cardiac activity, the left-sided chambers and the aorta should be vented once more. Attention is then directed to the pulmonary lesion, which will require repair by direct suture, lobectomy, or pneumonectomy as necessitated by the nature of the injury.
This condition arises whenever a portion of the chest wall becomes completely discontinuous from the rest of the rib cage. It usually results from blunt chest trauma in which several adjacent ribs are fractured on both sides of the sternum or, at least, at two locations on each of the ribs involved. This leads to a free-floating segment of the chest wall that positions itself in response to changes in pleural pressure rather than to the mechanical positions of the rest of the chest wall. The result is paradoxical movement of this portion of the chest wall. During spontaneous breathing, the flail segment moves inward with the negative pleural pressure of inspiration and moves outward with expiration. The diagnosis frequently is missed initially if one relies entirely on the detection of paradoxical movement of the chest wall because muscle spasm and pain restrict movement of the chest wall and make it very difficult to detect the paradoxical movement. This is particularly true in injuries involving the posterior thorax, where the muscle mass makes it even more difficult to detect paradoxical movement. Also, if the patient has been intubated and positive-pressure ventilation is instituted, paradoxical movement of the chest wall will not be seen. The presence of multiple adjacent rib fractures involving the same rib in different segments on chest x-ray would suggest the presence of flail chest even if it is not apparent clinically. The gas exchange abnormality is primarily due to the underlying lung contusion and not the flail per se. The degree of pulmonary and hemodynamic disability that arises is related to the extent of the flail, the degree of underlying lung contusion, and the restrictive effect of chest wall pain from the multiple fractures. There is, therefore, a wide spectrum of presentation of patients with flail chest.
In the severely hypoxemic patient with a large flail and/or hemodynamic instability, immediate endotracheal intubation and positive-pressure ventilation are indicated, with prompt chest tube insertion on the involved side to prevent a tension pneumothorax from developing on institution of positive-pressure ventilation. Patients who are able to maintain adequate oxygenation and ventilation with supplemental oxygen may be maintained without mechanical ventilation and endotracheal intubation, particularly if adequate pain control can be achieved. This may require frequent or continuous intravenous analgesia in the form of titrated fentanyl, morphine, or other agents. In other circumstances, epidural or, less preferably, intercostal blockade with long-acting local anesthetic agents may be used to control the pain. With adequate analgesia, it is possible to avoid endotracheal intubation and mechanical ventilation in most patients with flail chest.
Emergency thoracotomy is not required for treating flail chest. Also, mechanical fixation of the rib fractures usually is not necessary. There is still controversy as to whether formal thoracotomy and mechanical fixation of the fractured ribs should be considered at all in these patients. However, in situations where thoracotomy is required for other reasons, it may be appropriate to reduce and plate the fractures involved.
If a decision is made to ventilate the patient with a flail chest, the timing of weaning will not necessarily depend on disappearance of the paradoxical movement of the chest wall. Rather, weaning from the respirator may be initiated when the gas exchange abnormality associated with the underlying lung contusion is resolved. In fact, frequently these patients are weaned completely off respiratory support (with adequate pain control) when the lung contusion clears, even when residual paradoxical movement remains apparent for several weeks. A potential disadvantage of the nonsurgical and conservative nonventilating approach to flail chest is the acceptance of a high degree of ultimate chest wall deformity. However, these chest wall abnormalities are of questionable significance in terms of producing a long-term restrictive defect in these patients.
EMERGENCY THORACOTOMY
Improvement in trauma response time and prehospital resuscitation have resulted in many patients arriving in the emergency room “in extremis” with imminent cardiac arrest or with CPR in progress. There is thus an increasing role for thoracotomy in the emergency room as part of trauma resuscitation.
Emergency room thoracotomy allows:
Release of cardiac tamponade (especially in penetrating trauma)
Control of massive intrathoracic hemorrhage
Intrathoracic cardiac massage especially in the hypovolemic patient not responding to external cardiac massage
Thoracic aortic clamping for maintenance of perfusion to the heart and brain while controlling hemorrhagic sources distal to the thoracic aorta
Treatment of air embolism (Bronchovenous)
The highest survival rate in emergency thoracotomy is from the treatment of cardiac tamponade secondary to a penetrating mechanism. The key elements are early recognition, prompt decompression of the pericardial sac, and surgically correcting the source of the hemorrhage. Utilization of FAST (Focused Assessment Sonogram in Trauma) allows early recognition of hemopericardium. Hypotension, distended neck veins, and hemopericardium confirm cardiac tamponade.
Phases in Cardiac Tamponade: First phase: Initially cardiac output is maintained by an increase in the heart rate.
Second phase: Cardiac output decreases but blood pressure is maintained by an increase in peripheral vascular resistance and a decrease in pulse pressure secondary to catecholamine release. In these two phases, there is time to take the patient to the operating room, which is more ideally suited for thoracotomy. Airway control and volume infusion are initiated prior to the operating room thoracotomy.
Third phase: In this phase there is profound hypotension, which makes it unsafe to transport the patient to the operating room. Emergency room thoracotomy for decompression of the pericardial sac and identification and treatment of the cardiac laceration is warranted.
Control of Intrathoracic Hemorrhage: Less than 5% of intrathoracic hemorrhage is massive requiring emergency room thoracotomy. The mechanism is usually penetrating. Emergency room thoracotomy allows temporary clamping of the pulmonary hilum, clamping and repair of major vascular sources of hemorrhage as well as repair of cardiac wounds.
Open Cardiac Massage:
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


