Thrombocytopenia is a very common occurrence in the intensive care unit (ICU), occurring in as many as 60% of patients. The normal platelet count ranges between 150,000 and 450,000/µL. In the ICU, it is important to recognize that the absolute platelet count is important, but trends in the platelet count, specifically a decline by more than one-half, may be evidence of a serious clinical problem such as heparin-induced thrombocytopenia (HIT), which requires urgent attention. A systematic approach to the diagnosis allows for the common causes to be detected early and enables rational use of platelet transfusions (Algorithm 62.1). Platelet survival in the circulation is approximately 7 to 10 days, and one-third of the platelets are sequestered in the spleen under normal circumstances.
Recognition of thrombocytopenia normally occurs after a complete blood count is drawn, but it is important to remember that mucocutaneous bleeding is a classic sign of thrombocytopenia. Bleeding from thrombocytopenia normally occurs only once the platelet count is <50,000/µL in postsurgical patients; spontaneous bleeding can occur with counts <5000/µL. The diagnostic approach starts with a thorough history and physical examination, followed by examination of the peripheral smear. A pathophysiologic approach to thrombocytopenia enables all common causes to be rapidly screened for and facilitates recognition of potential causes (Table 62.1). Careful attention should be paid to prescription and over-the-counter drugs (Table 62.2).
The common causes of thrombocytopenia in an ICU setting are as follows:
Clinical recognition of the cause is vital, as the therapies differ considerably depending on the etiology. For example, a patient with thrombocytopenia secondary to bleeding should be treated with platelets compared with a patient with TTP/HUS, in whom platelet transfusion is generally contraindicated. A few common conditions will be discussed, and readers are encouraged to refer to Suggested Reading for further details.
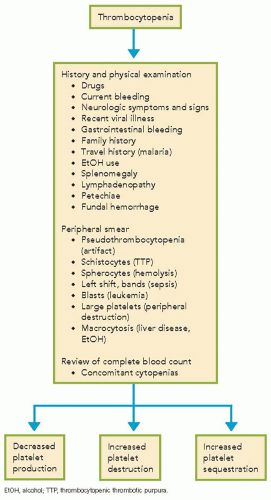
ALGORITHM 62.1 Diagnostic Algorithm for Thrombocytopenia
TABLE 62.1 Pathophysiologic Classification of Thrombocytopenia