5 Thorax and Abdomen !++ R 2 times a week, up to 8 weeks MM, ThE, MET !++ R 3 times a week, up to 8 weeks PhysApps, ThE, Met, Chiro !++ R 2 times a week, up to 8 weeks ThE, PIR, MM ! +++ R1–2 times per week, up to 4 weeks MM, Acu, FMA, Med
 Complex Pain
Complex Pain
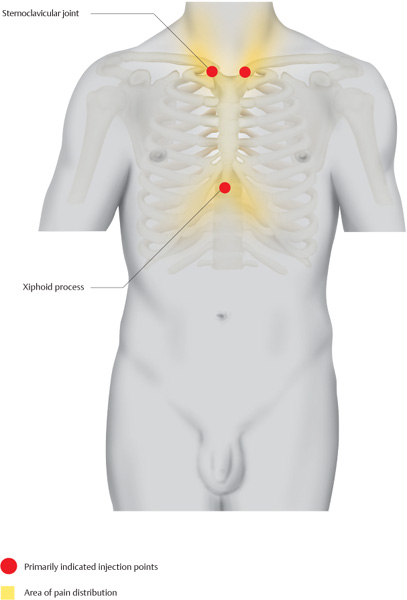
Xiphoid–Sternum–Clavicle Triangle
Indications
 Sternum pain, painful sternoclavicular joint, painful sternoclavicular joint in the case of arthrosis, and conditions following clavicle fracture
Sternum pain, painful sternoclavicular joint, painful sternoclavicular joint in the case of arthrosis, and conditions following clavicle fracture
 Emphysematous thorax including xiphoid pain
Emphysematous thorax including xiphoid pain
Differential Diagnoses
 Intestinal and mediastinal affections
Intestinal and mediastinal affections
 Respiratory disorders
Respiratory disorders
Material
 Local anesthetic: 2.5 mL
Local anesthetic: 2.5 mL
 Needle: 0.6 × 30 mm
Needle: 0.6 × 30 mm
Technique
 The sternoclavicular joint is easily palpable. The clavicle is palpated up to its medial sternal end, where the palpating finger drops into a depression. The joint line can be palpated by moving the arm. The needle is inserted vertically 0.5 cm and 0.5 mL of a local anesthetic is injected.
The sternoclavicular joint is easily palpable. The clavicle is palpated up to its medial sternal end, where the palpating finger drops into a depression. The joint line can be palpated by moving the arm. The needle is inserted vertically 0.5 cm and 0.5 mL of a local anesthetic is injected.
 This procedure is performed at both sternoclavicular joints and is followed by locating the xiphoid; this bone–cartilage process is usually distinctly pressure sensitive at one spot. The needle is inserted vertically 1 cm (observe the depth of insertion) and 1.5 mL of a local anesthetic is injected.
This procedure is performed at both sternoclavicular joints and is followed by locating the xiphoid; this bone–cartilage process is usually distinctly pressure sensitive at one spot. The needle is inserted vertically 1 cm (observe the depth of insertion) and 1.5 mL of a local anesthetic is injected.
Risks
 If the needle is inserted excessively deep and the joint line is missed, a pneumothorax may occur at the sternoclavicular joint.
If the needle is inserted excessively deep and the joint line is missed, a pneumothorax may occur at the sternoclavicular joint.
 If the injectable is administered excessively deep at the xiphoid process, abdominal organs may be injured.
If the injectable is administered excessively deep at the xiphoid process, abdominal organs may be injured.
Concomitant Therapies
 Mobilization of the sternoclavicular joint using manual therapy
Mobilization of the sternoclavicular joint using manual therapy
 Postisometric relaxation of the rectus abdominis
Postisometric relaxation of the rectus abdominis
 Consistently exercising the levator scapulae
Consistently exercising the levator scapulae
 Stretching treatment for the shortened pectoralis major
Stretching treatment for the shortened pectoralis major
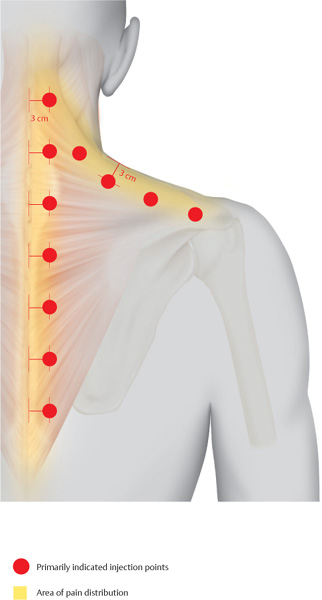
Interscapular Pain
Indications
 Interscapular pain
Interscapular pain
 Thoracic syndrome accompanying obstructive respiratory disorders, for example, bronchial asthma
Thoracic syndrome accompanying obstructive respiratory disorders, for example, bronchial asthma
Differential Diagnoses
 Affections of the pleural dome
Affections of the pleural dome
 Cardiac disorders
Cardiac disorders
Material
 Local anesthetic: 5 mL
Local anesthetic: 5 mL
 Needle: 0.6 × 30 mm
Needle: 0.6 × 30 mm
Technique
 A vertical line is drawn 3 cm lateral to the spinous processes. Along this line, the needle is inserted vertically every 2 cm.
A vertical line is drawn 3 cm lateral to the spinous processes. Along this line, the needle is inserted vertically every 2 cm.
 At each site, an intracutaneous quaddle containing 0.5 mL of a local anesthetic is set, then the needle is advanced 1 cm and a further 0.5 mL of a local anesthetic is injected. Injections follow the pathway of the bladder meridian.
At each site, an intracutaneous quaddle containing 0.5 mL of a local anesthetic is set, then the needle is advanced 1 cm and a further 0.5 mL of a local anesthetic is injected. Injections follow the pathway of the bladder meridian.
Risks
 If the needle is advanced excessively, there may be the rare occurrence of a pneumothorax, especially at the vertex of the kyphosis; therefore, the depth of insertion must be observed.
If the needle is advanced excessively, there may be the rare occurrence of a pneumothorax, especially at the vertex of the kyphosis; therefore, the depth of insertion must be observed.
Concomitant Therapies
 Local warm peloid application, combined with mobilization of the subscapularis and lateral traction mobilization
Local warm peloid application, combined with mobilization of the subscapularis and lateral traction mobilization
 Relaxation massages, acupuncture treatments
Relaxation massages, acupuncture treatments
 Hot jet blitz to the back, according to Kneipp
Hot jet blitz to the back, according to Kneipp
 Chiropractic therapy
Chiropractic therapy
 Therapy through Muscles, Tendons, and Ligaments
Therapy through Muscles, Tendons, and Ligaments
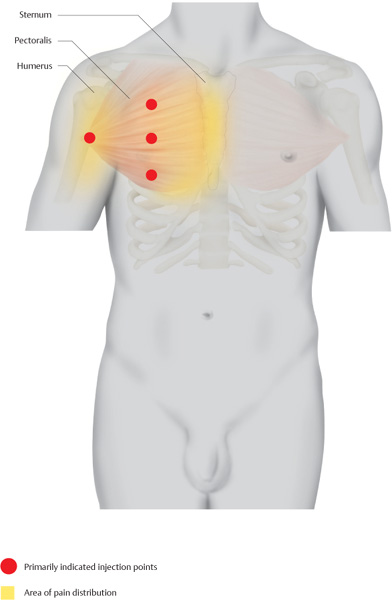
Pectoralis Major
Indications
 Painful shortening of the pectoralis major accompanied by myotendinous irritation
Painful shortening of the pectoralis major accompanied by myotendinous irritation
 Adjuvant treatment in emphysema
Adjuvant treatment in emphysema
 Adjuvant treatment in painful sternocostal joints
Adjuvant treatment in painful sternocostal joints
 Adjuvant treatment in respiratory disorders
Adjuvant treatment in respiratory disorders
Material
 Local anesthetic: 4 mL
Local anesthetic: 4 mL
 Needle: 0.6 × 30 mm
Needle: 0.6 × 30 mm
Technique
 Beginning at the mamillary line, the injectable is administered intramuscularly every 3 cm along a line that curves slightly laterally. Frequently, distinct pressure-sensitive myogeloses are found on that line. These points are fixed with the two-finger technique, the needle is inserted vertically 1 cm, and 1 mL of the injectable is administered.
Beginning at the mamillary line, the injectable is administered intramuscularly every 3 cm along a line that curves slightly laterally. Frequently, distinct pressure-sensitive myogeloses are found on that line. These points are fixed with the two-finger technique, the needle is inserted vertically 1 cm, and 1 mL of the injectable is administered.
 In addition, a local anesthetic is always injected into the attachment at the upper arm. The inferior border of the pectoralis major is traced to the humerus. The needle is inserted 1 cm superiorly toward the bone until bone contact is made. After the needle has been retracted 1–2 mm, 1 mL of a local anesthetic is injected.
In addition, a local anesthetic is always injected into the attachment at the upper arm. The inferior border of the pectoralis major is traced to the humerus. The needle is inserted 1 cm superiorly toward the bone until bone contact is made. After the needle has been retracted 1–2 mm, 1 mL of a local anesthetic is injected.
Risks
 None
None
Concomitant Therapies
 Especially physical therapy, including stretching and postisometric relaxation of the pectoralis major and pectoralis minor
Especially physical therapy, including stretching and postisometric relaxation of the pectoralis major and pectoralis minor
 Mobilization of the costovertebral joints using manual therapy
Mobilization of the costovertebral joints using manual therapy
 Medical assessment of the workplace or adequate assessment of motion sequences during athletic activities, if applicable
Medical assessment of the workplace or adequate assessment of motion sequences during athletic activities, if applicable
 Friction massage of the pectoralis major
Friction massage of the pectoralis major
Sternocostalis
Indications
 Diffuse pectoral pain
Diffuse pectoral pain
 Tietze syndrome
Tietze syndrome
 Sternocostal joint dysfunctions
Sternocostal joint dysfunctions
 Pain syndromes following rib fractures
Pain syndromes following rib fractures
Material
 Local anesthetic: 0.5 mL per sternocostal joint
Local anesthetic: 0.5 mL per sternocostal joint
 Needle: 0.4 × 20 mm
Needle: 0.4 × 20 mm
Technique
 Initially, the sternum is palpated. From there, the finger moves laterally to the palpable sternocostal joint. The precise position is confirmed by having the patient inhale and exhale deeply; this allows the physician to palpate the motion within the sternocostal joint. The needle is inserted vertically 0.5 cm and 0.5 mL of a local anesthetic is injected.
Initially, the sternum is palpated. From there, the finger moves laterally to the palpable sternocostal joint. The precise position is confirmed by having the patient inhale and exhale deeply; this allows the physician to palpate the motion within the sternocostal joint. The needle is inserted vertically 0.5 cm and 0.5 mL of a local anesthetic is injected.
 If necessary, the joint line is felt for after the needle tip has made bone contact.
If necessary, the joint line is felt for after the needle tip has made bone contact.
Risks
 If the needle is advanced excessively, the pleura or the left pericardium may be injured; therefore, the depth of insertion must be observed.
If the needle is advanced excessively, the pleura or the left pericardium may be injured; therefore, the depth of insertion must be observed.
Concomitant Therapies
 Mobilization and manipulation of the sternocostal joint using manual therapy
Mobilization and manipulation of the sternocostal joint using manual therapy
 Acupuncture on the kidney channel, especially KI-22–KI-27, in combination with BL-11–BL-19
Acupuncture on the kidney channel, especially KI-22–KI-27, in combination with BL-11–BL-19
 Friction massage of the intercostals, topical anti-inflammatory therapy
Friction massage of the intercostals, topical anti-inflammatory therapy

Rectus Abdominis
Indications
 Myotendinous complaints in the muscle area
Myotendinous complaints in the muscle area
 Diffuse complaints in the upper abdomen, subcostally radiating complaints accompanied by back pain
Diffuse complaints in the upper abdomen, subcostally radiating complaints accompanied by back pain
 Adjuvant treatment in small intestine dysfunction
Adjuvant treatment in small intestine dysfunction
Material
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


