19 The Treatment of Pain Through Chinese Scalp Acupuncture
Around 1950, various famous Chinese physicians introduced Western neurophysiology into acupuncture fields and explored the relationship between the brain and human body. Although there were several hypotheses, it took acupuncture practitioners roughly 20 years before they accepted a central theory that incorporated brain functions into the Chinese meridian theories. Dr. Jiao Shunfa, a neurosurgeon in Shanxi province in China, is the official recognized founder of Chinese scalp acupuncture.1 Starting in 1972, he systematically undertook the scientific exploration and charting of scalp correspondences for the first time in more than 2500 years of acupuncture history. Dr. Jiao combined a modern understanding of neuroanatomy and neurophysiology with traditional techniques of Chinese acupuncture to develop a radical new tool for treating the central nervous system. At the time, scalp acupuncture was primarily used to treat paralysis and aphasia due to stroke. Dr. Jiao’s discovery was investigated, acknowledged, and formally recognized by the acupuncture profession in a national unified acupuncture textbook, Acupuncture and Moxibustion in 1977.
In 1987, scalp acupuncture began to gain international recognition at the first International Acupuncture and Moxibustion Conference held in Beijing. In 1989, Dr. Jason Jishun Hao brought scalp acupuncture to the United States. Since then, Dr. Hao has trained hundreds of acupuncture practitioners and treated thousands of patients with disorders of the central nervous system in the United States. After its introduction in the United States, the techniques and applications of scalp acupuncture have been expanded and developed through further research and experience. Studies and research on scalp acupuncture continue to show positive results in treating the disorders of the central nervous system.2
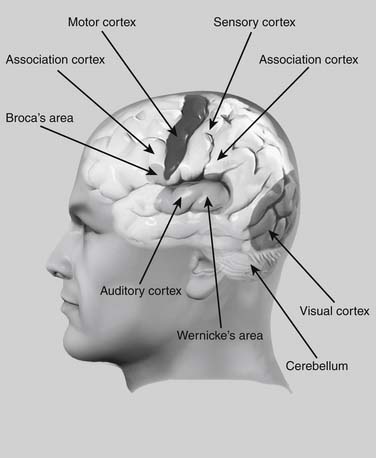
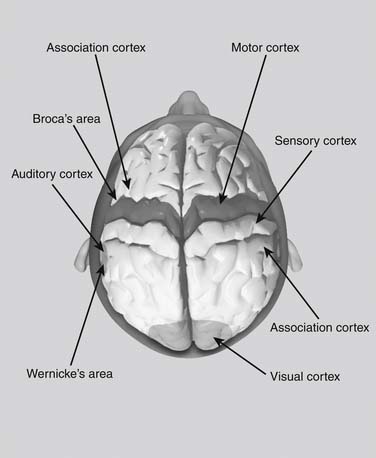
Scalp acupuncture is based on a reflex somatotopic system organized on the surface of the scalp. Scalp acupuncture consists of needling areas versus points on the skull according to the brain’s neuroanatomy and neurophysiology. Unlike acupuncture, where one needle is inserted into a single point, in scalp acupuncture needles are subcutaneously inserted into whole sections of various zones. These sections are the specific zones through which the functions of the central nervous system, endocrine system, and meridians are transported to and from the surface of the scalp. From a Western perspective, these areas correspond to the cortical areas of the cerebrum and cerebellum, which are responsible for central nervous system functions such as motor function, speech, and balance (Figs. 19-1 and 19-2).
In a recent study by the author, scalp acupuncture was used to treat seven patients with phantom limb pain at Walter Reed Army Medical Center in Washington, D.C.3 After only one treatment per patient, three of the seven patients instantly felt pain relief and showed significant improvement, whereas three patients showed some improvement, and only one patient showed no improvement (see later). Because of the limited numbers of patients, this needs to be replicated on a larger scale. It nevertheless shows the potential efficacy of scalp acupuncture in treating phantom pain.
Scalp acupuncture can provide solutions in situations where Western medicine solutions are limited or entail too much risk. This chapter will show the scope of scalp acupuncture in treating many kinds of diseases. This research is derived from many years of clinical experience and can be used as the foundation for future clinical practice and research.
Location and Indication
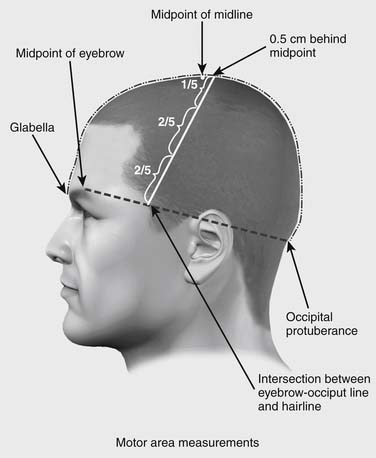
Precise location of Chinese scalp acupuncture areas requires identification of two imaginary lines on the head. The anterior-posterior line runs along the centerline of the head. The midpoint of the skull is located at the midpoint between the occipital protuberance and the glabella, midway between the eyebrows. The second line, the horizontal line, runs from the highest point of the eyebrow to the occipital protuberance. Where this line intersects the anterior hairline defines the lower point of the motor area (Fig. 19-3). In patients without a definite hairline, an alternative method for locating this point is to draw a vertical line up from acupuncture point ST-7 until it intersects the line from the brow to the occipital.
Motor Area Location
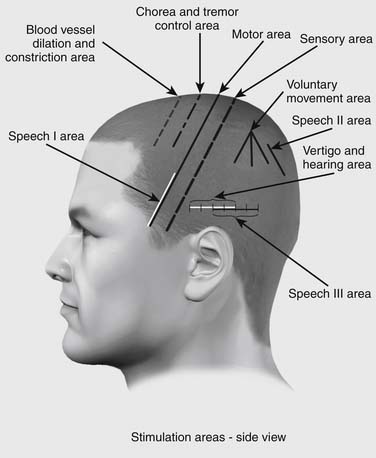
The motor area is located on the projective area of the scalp corresponding to the precentral gyrus of the frontal lobe. The motor area is located in a strip beginning at the midline at a point 0.5 cm posterior to the previously located midpoint of the head, along the anterior-posterior line.4 The motor area runs from this point obliquely down to the point where the eyebrow-occipital line intersects the anterior hairline (Fig. 19-4). The line of the motor area determines the angle and location of several other areas, such as the sensory area and chorea and tremor area.
The motor area is divided into three regions according to the homunculus projection.5 In order to correctly locate those three regions, the whole motor area is first equally divided into fifths. Then three regions are measured as Upper one-fifth region, Middle two-fifths region, and Lower two-fifths region. The Upper one-fifth region is used to treat contralateral movement dysfunction of the lower extremity, trunk, spinal cord, and neck. The Middle two-fifths region is used to treat contralateral movement dysfunction of the upper extremity. The Lower two-fifths region is used to treat bilateral movement dysfunction of the face and head. These areas are used to affect the contralateral side of the body. The direction of needling is usually from the upper part of the area downward, penetrating to the entire area.
Motor Area Indications
Indications to apply needles in the motor area are: paralysis or weakness in the face, trunk, or limbs caused by stroke; multiple sclerosis; traumatic paraplegia; acute myelitis; progressive myotrophy; neuritis; poliomyelitis; post-polio syndrome; periodic paralysis; hysterical paralysis; Bell’s palsy; spinal cord injury; traumatic brain injury; and brain surgery.
Sensory Area Location
The sensory area is located on the projective area of the scalp corresponding to the post-central gyrus of the frontal lobe. The sensory area is one of the most commonly used in Chinese scalp acupuncture. It is located parallel to the motor area, 1.5 cm posterior to the motor area (see Fig. 19-4).
Additional Areas of the Cortex
Tremor and Chorea Area
The Chorea and Tremor Area is located parallel to the motor area, 1.5 cm anterior to the motor area (see Fig. 19-4). It runs 4 cm and starts 1 cm anterior to the Midpoint at its upper point. This area is always needled bilaterally and is used for any involuntary motor activity. This is the primary area for the treatment for Parkinson’s disease, tremor, shaking of the head, body, or extremities, and chorea. This area is also very effective for treating patients with muscular tension and tightness in any part of the body. The direction of needling is usually from the upper part of the area downward, penetrating to the entire area.
Vascular Dilation and Constriction Area
This area is also parallel to the motor area, 1.5 cm anterior to the chorea and tremor area, or 3 cm anterior to the motor area (see Fig. 19-4). This area is also always needled bilaterally and can be used for essential hypertension, cortical edema, and other autonomic vascular dysfunctions. The direction of needling is usually from the upper part of the area downward, penetrating the entire area.
Vertigo and Hearing Area
This area is located over temporal lobe in the lateral side of the head. It is on the horizontal line and totals 4 cm.6 It starts 1.5 cm superior to the apex of the auricle of the ear at its middle point, and extends 2 cm anterior and 2 cm posterior to the middle point (see Fig. 19-4). This area is also needled bilaterally and can be needled in either direction. This is a very useful area for treating vertigo, dizziness, Meniere disease, tinnitus, hearing loss, and hearing hallucination.
Speech I Area
There are three speech areas. Speech I area is located in the posterior third of the gyrus frontalis inferior over the frontal lobe, and controls groups of muscles for speech and phonation. Speech I area corresponds to Broca’s speech area of the frontal lobe, which controls the muscles of the tongue and mouth that form speech. Speech I area overlaps the lower 2/5 40% of the motor area (see Fig. 19-4). The major indication for Speech I is in the presence of motor aphasia after stroke or brain injury, where the muscles of speech and vocalization have been paralyzed. This area is needled bilaterally for motor aphasia. The direction of needling is usually from the upper part of the area downward, penetrating the entire area.
Speech II Area
This area lies over the reading and comprehension part of the parietal lobe, and is located by finding the parietal tubercle. From the parietal tubercle, run a line parallel to the anterior-posterior line 2 cm posteriorly. Using this as the starting point, the Speech II area runs 3 cm in length, parallel to the anterior-posterior line (see Fig. 19-4). This area is used bilaterally for nominal aphasia—the inability to name objects. In this disorder, the patient can describe an object, but cannot produce the noun. The direction of needling is usually from the upper part of the area downward.
Speech III Area
This overlies Wernicke’s area of the temporal lobe, and overlaps the posterior half of the vertigo and hearing area. It lies on the same horizontal line 1.5 cm superior to the apex of the auricle but begins at the midpoint of the vertigo and hearing area directly above the auricle and runs 4 cm posteriorly (see Fig. 19-4). It is used bilaterally for treatment of expressive aphasia, where the patient can articulate words, but the words don’t make sense. The direction of needling can go either from the left part to the right or from right to left side, penetrating the entire area.
Praxis Area
This is an area used uncommonly. Starting from the parietal tubercle, the praxis area joins three lines, one running straight downward, and the other two at a 40-degree angle anterior and posterior to the vertical line (see Fig. 19-4). This area is used for apraxia—the inability to execute certain fine motor activities such as buttoning a shirt.
Vision Area
The vision area is located over the occipital lobe on the posterior aspect of the head. It starts on a horizontal line at the level of the occipital protuberance. The vision area starts at a point 1 cm lateral to the occipital protuberance and runs upward for 4 cm, parallel to the anterior-posterior line (Fig. 19-5). The vision area is often needled bilaterally. Unlike other scalp areas in Chinese acupuncture, the vision area must be needled from the top down. Needling from below upward incorrectly has the risk for causing injury to the medulla. Indications for needling are vision loss due to stroke or brain injury, visual field loss, visual hallucination, and nystagmus.
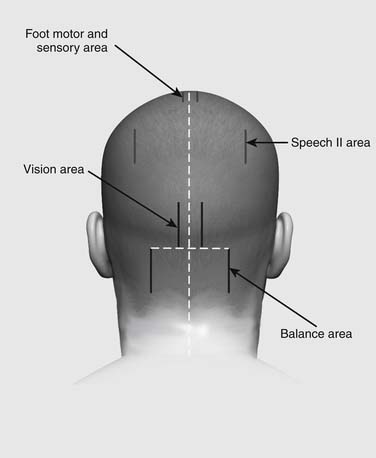
Balance Area
The balance area is located over the cerebellum. It starts on a horizontal line at the level of the occipital protuberance. The balance area starts from a point 3.5 cm lateral to the occipital protuberance and runs 4 cm inferiorly (see Fig. 19-5).








