Introduction
The symptom of pain is one of the commonest reasons for consulting a physiotherapist and the treatment of pain, especially musculoskeletal pain, occupies the majority of clinician time in a busy outpatient department. A physiotherapist can be involved at all durations of injury, from acute injury on the sports field to chronic pain management programmes.
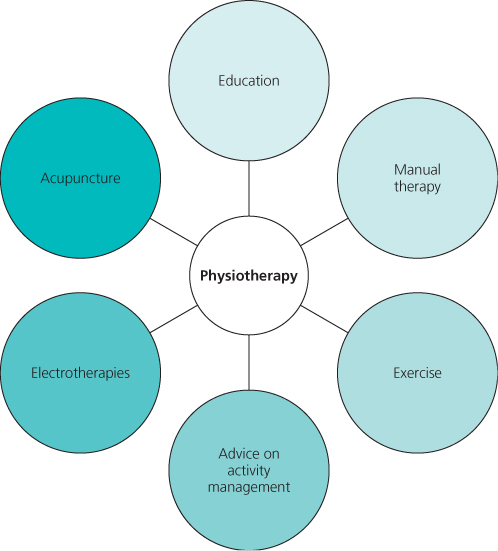
Physiotherapy covers a variety of treatments, some which are well supported by evidence and others which have not been subjected to close scrutiny. It would be a mistake to see physiotherapy as consisting of one or other of these treatments, rather than a package of care (Figure 17.1). At its best physiotherapy is a package of rehabilitation but time constraints and the knowledge, beliefs and experience of the individual therapist can mitigate against the provision of optimal treatment. Most physiotherapy is concerned with the subacute and, especially, the chronic phase of injury; the techniques and treatment are discussed further here.
Figure 17.1 Physiotherapy is a package of care that may encompass a range of therapies, with some examples shown here.
Physiotherapy in Acute Injury
The aim of physiotherapy for acute pain is to manage the underlying inflammatory process to encourage healing and early restoration of function.
Movement restriction is recommended in the very early stage of an acute injury and this is achieved by the use of splints and non-elastic strapping or bandaging (Figures 17.2 and 17.3). The latter also provides compression to help reduce swelling but must be applied carefully and reviewed regularly to prevent further complications. Cold therapy is applied immediately to reduce pain and swelling. At its simplest cold therapy is ice alone but there are a number of sophisticated cold therapy devices which can be incorporated into splints to provide both cold therapy and compression.
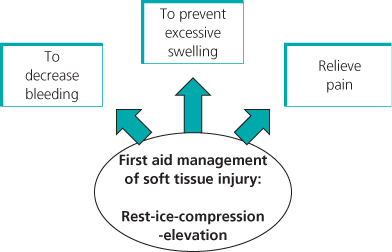

Ice may be applied repeatedly over one or two weeks to keep swelling under control. It is often applied after exercise in the early stages of rehabilitation. Ice cools the tissue and lowers tissue metabolism in the immediate stages after injury, it reduces hypoxic cell death and relieves pain through reducing neuronal activity. Ice must be applied early; a delay of 24 hours will reduce the effectiveness of ice therapy. Early mobilisation is recommended once the acute stage of healing starts to subside. This will of course depend on the severity of the injury.
Electrotherapies
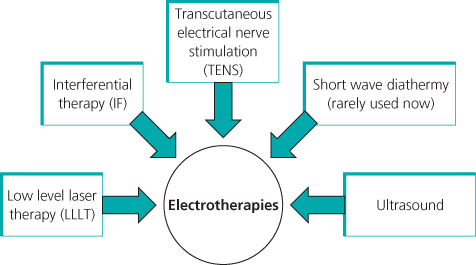
A range of electrotherapies can be used in the management of both acute and chronic injury (Figure 17.4). The research evidence for many of these treatments is scant, often with conflicting results. The main problem with the research is the lack of scientific rigour in many of the studies.
Low Level Laser Therapy (LLLT)
Reviews of the literature have suggested that there is some evidence for the use of LLLT in people with chronic joint problems, such as osteoarthritis, and some myofascial pain problems (Figure 17.5). The mode of action is unclear but laboratory studies have suggested that LLLT can modulate pain through reducing pro-inflammatory cytokines and reduce the development of oedema. The effect on non-specific low back pain and other musculoskeletal pain problems is inconclusive and generally laser therapy has gradually diminished in use, at least in the National Health Service in the United Kingdom, because of a lack of clear evidence of effect.

Transcutaneous Electrical Nerve Stimulation (TENS)
Transcutaneous Electrical Nerve Stimulation (TENS) will be familiar to most clinicians; these small portable devices are easily available and widely used by patients who often buy them from pharmacists. The device emits an electrical current which can be varied. Clinically TENS is considered worth trying in a wide variety of musculoskeletal pain conditions because it is simple to use, has low risk and only a short trial is required to evaluate the effectiveness in an individual patient.
In the acute pain setting, studies have demonstrated no advantage of TENS over routine analgesia in post-operative pain; however, subsequent reviews considering the quality of the clinical application of TENS have concluded there is a medication sparing role for TENS and it could be considered as an adjunct to routine analgesia where patients wish to restrict their medication consumption.
The mechanism of action and practical use of TENS in chronic pain is covered further in Chapter 18.
Interferential Therapy
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


