1 The history of frequency-specific microcurrent
The history of electromagnetic therapies
Starting in the late 1800s there was a tremendous upwelling of interest in electromagnetism and electrical effects. In the early 1900s, medical physicians and osteopaths were interested in using electromagnetic therapies and frequencies as a way of treating patients. The devices and techniques were used by thousands of doctors but were not accepted by the medical establishment. Albert Abrams, MD used electromagnetic therapies in his San Francisco clinic from 1914 until his death in 1937. He founded the Electromedical Society and the journal Electromedical Digest as a way for practitioners to communicate and share their research and treatment findings (ERA 1980). In 1934 the American Medical Association, in its efforts to standardize medical education and treatments, decreed that drugs and surgery were the accepted tools of medicine and anyone using electromagnetic therapies would lose their license to practice which at that time was granted by the AMA. The research and clinical use of electromagnetic therapies in medicine came to a halt and by the early 1950s the necessary devices were rendered illegal in the United States by the FDA, after which, electromedical practice gradually died out although the early devices remained in use in private medical and osteopathic practices around the US, Canada and England.
First uses of microcurrent and the frequencies
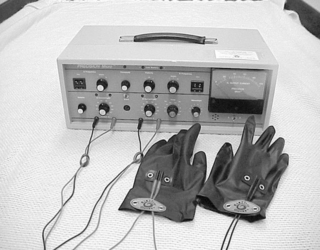
Microcurrent was introduced in the United States as a physical therapy modality in the late 1970s by a chiropractor and acupuncturist Dr. Thomas Wing. Dr. Wing used four low frequencies such as .3Hz, .6Hz, 10Hz, and 30Hz delivered with single channel microcurrent unit using cotton tipped probes and eventually a double channel microcurrent called the “Myomatic I” (I = interferential). Because of its ability to increase ATP production (Cheng 1982) microcurrent was being used by Dr. Wing and others to increase the rate of healing in injured athletes, to control pain, to increase the rate of fracture repair and wound healing and to treat myofascial pain.