1. About 45% to 75% of ulcerative colitis patients eventually need surgery. Indications are divided into emergency, urgent, and elective. Emergency procedures are done for life-threatening complications of fulminant colitis unresponsive to medical treatment. Urgent surgery is indicated in patients with severe ulcerative colitis who do not respond to inpatient intensive medical treatment.
2. The missing nerve supply (Auerbach plexus and Meissner plexus) in Hirschsprung disease results in spasm of the bowel in the affected area and distension proximal to the affected area, with retention of feces and intestinal obstruction with constipation.
3. Pediatric dysmotility disorders include gastroesophageal reflux disease (GERD), esophageal achalasia, gastroparesis, Hirschsprung disease, chronic intestinal pseudo-obstruction, and constipation. Constipation is a common pediatric disorder and may have substantial morbidity medically as well as socially.
4. Malformations of the anus are usually a result of abnormal development of the proctodeum. Atresias, stenoses, and fistulas of the rectum result from an abnormality in the resolution of the anorectal membrane.
DISORDER: Inflammatory bowel diseases: Crohn disease, ulcerative colitis
BACKGROUND: The inflammatory bowel diseases (IBD)—Crohn disease and ulcerative colitis—are chronic and relapsing inflammatory conditions of either (1) the colon sparing the upper gastrointestinal (GI) tract (chronic ulcerative colitis) or (2) the entire alimentary tract (mouth to anus) (Crohn disease) with a large number of patients having terminal ileitis (1–3). While not technically a disorder of the hindgut, both IBD are placed here in order to facilitate comparison. Unfortunately, the incidence is on the rise for both, and increasing encounters with a variety of clinicians, especially in pediatric IBD, often requires the involvement of pediatric anesthesiologists for endoscopic as well as surgical procedures. In about 10% of patients, indeterminate colitis is the “working” diagnosis because a definitive diagnosis is not possible.
CLINICAL FEATURES (Table 23.1)
Chronic ulcerative colitis: Typically begins as rectal disease extending proximally for a variable distance. Its incidence is geographically variable (1.5:10,000 in the United States; 0.1:10,000 in Japan and South Africa). A family history of IBD is the most important independent risk factor (first-degree relatives: 5.7% to 15.5%). Ashkenazi Jews have a rate three to five times higher than that of other ethnic groups. These differences are lessening, which suggests an environmental effect as well. Clinical manifestations include bloody diarrhea with mucus, tenesmus, urgency, crampy abdominal pain, and nocturnal bowel movements. Fulminant colitis may present with fever, severe anemia, hypoalbuminemia, leukocytosis, and frequent stooling. Anorexia, growth failure, and weight loss may be present. Prolonged remission may follow the initial presentation in 5%, or the exacerbation may persist requiring urgent surgery. The risk of colon cancer begins to rise (0.5% to 1.0%/year) after about 10 years of disease.
CLINICAL PEARL
1. Clinical manifestations of ulcerative colitis include bloody diarrhea with mucus, tenesmus, urgency, crampy abdominal pain, and nocturnal bowel movements.
2. Fulminant colitis may present with fever, severe anemia, hypoalbuminemia, leukocytosis, and stool frequency. Anorexia, growth failure, and weight loss may be present.
TABLE 23.1 Comparison of irritable bowel disorders
Feature | Crohn disease | Ulcerative colitis |
Rectal bleeding | + | +++ |
Abdominal mass | +++ | – |
Rectal disease | +++ | +++ |
Ileal involvement | +++ | – |
Perianal disease | +++ | – |
Strictures | +++ | – |
Fistula | +++ | – |
Discontinuous (skip) lesions | +++ | – |
Transmural involvement | +++ | – |
Crypt abscesses | + | +++ |
Granulomas | +++ | – |
Risk for colon cancer | + | +++ |
Pyoderma granulosum | + | ++ |
Erythema nodosum | +++ | + |
Mouth ulcers | +++ | – |
Cholangitis | + | + |
Stroke | + | + |
The diagnosis is based on a typical history and presentation. Colonoscopy should not be performed if fulminant colitis is suspected because of the risk of initiating toxic megacolon or causing a perforation. Biopsy during nonfulminant stages typically reveals findings of acute and chronic mucosal inflammation with cryptitis, crypt abscesses, separation of crypts by inflammatory cells, edema, mucus depletion, and crypt branching. Inflammation in ulcerative colitis is characteristically restricted to the mucosal surface; full-thickness involvement of the bowel wall suggests Crohn disease.
CLINICAL PEARL Biopsy during nonfulminant stages typically reveals findings of acute and chronic mucosal inflammation with cryptitis, crypt abscesses, separation of crypts by inflammatory cells, edema, mucus depletion, and crypt branching.
Medical treatment of chronic ulcerative colitis consists of sulfasalazine, mesalazine (the active moiety of sulfasalazine) initially, followed by corticosteroids, immunosuppressive drugs, and monoclonal antibodies to tumor necrosis factor (TNF)-α. The effects of chronic steroid administration (growth retardation, adrenal suppression, cataracts, osteopenia, aseptic necrosis of the head of the femur, glucose intolerance, risk of infection, cosmetic effects) have to be kept in mind. Patients with corticosteroid-dependent disease, and those who relapse despite optimum doses of mesalazine, can be treated with azathioprine or mercaptopurine with modest additional efficacy. No improvement after 3 to 5 days of intravenous steroids during a severe flare is an indication to start rescue treatment. Infliximab, cyclosporine, tacrolimus, and surgery are all effective rescue strategies (4).
Eventually, anywhere from 45% to 75% of ulcerative colitis patients need surgery.
CLINICAL PEARL Eventually, anywhere from 45% to 75% of ulcerative colitis patients need surgery.
Crohn disease: Characterized by transmural involvement of gastrointestinal mucosa at any point in the alimentary tract, typically eccentric and segmentally distributed, often with skip areas (5). Particularly with children, the initial presentation usually involves ileum and colon but can involve the small bowel alone. As with ulcerative colitis, Crohn disease diagnosis usually peaks in late adolescence. The incidence of Crohn disease has been increasing over the past 15 years, with an incidence of about 0.3 to 0.4:10,000.
CLINICAL PEARL Characterized by transmural involvement of gastrointestinal mucosa at any point in the alimentary tract, typically eccentric and segmentally distributed, often with skip areas.
CLINICAL PEARL Particularly with children, the initial presentation usually involves ileum and colon but can involve the small bowel alone.
Children with ileocolitis typically have crampy abdominal pain and diarrhea, sometimes with blood. Pain may be right lower quadrant in the presence of ileitis alone. Fever, malaise, and easy fatigability are common. Perianal disease (tags, fistula, abscess) is common. Partial small bowel obstruction due to luminal narrowing may occur. Enteroenteric or enterovesical fistulization may occur with the anticipated symptoms depending on the location of the communication, and enterocutaneous fistulas may occur at the site of previous surgery. Evaluation may require radiological (contrast, ultrasound, computed tomography, magnetic resonance imaging [MRI]) or gastrointestinal (GI) studies.
Once the diagnosis is established, medical treatment is directed toward symptom relief. Prednisone is used for small-bowel disease, and is effective in inducing remission in most patients. Long-term steroid use is generally not recommended, however, because of the adverse cosmetic effects, suppression of growth in children, and osteopenia. Sulfasalazine and mesalazine are used to treat mild to moderate disease and to maintain remission. Antibiotic treatment with metronidazole and ciprofloxacin are also useful in mild to moderate disease, especially in patients with perianal disease. Immunosuppressive drugs such as 6 mercaptopurine and azathioprine are used for patients with steroid dependency, extensive small-bowel disease, history of previous resections, gastroduodenal disease, and perianal disease/refractory fistulas. Methotrexate and cyclosporine have also been used in these extreme circumstances as have biologic anti-TNF-α therapy such as infliximab. Nutritional therapy via nasogastric tube or gastrostomy-administered elemental or semi-elemental diets at night has also been utilized, as has total parenteral nutrition.
CLINICAL PEARL Once the diagnosis is established, medical treatment is directed toward symptom relief.
PHYSIOLOGIC CONSIDERATIONS
1. Constipation/obstipation/diarrhea/abdominal pain/distension
2. Fever
3. Anemia (iron deficiency; anemia of chronic disease)
4. Hypoalbuminemia, hypoproteinemia
5. Physiologic effects of drug therapy
6. Emotional distress of chronic disease
SURGICAL REPAIR
ULCERATIVE COLITIS
About 45% to 75% of patients eventually need surgery. Indications are divided into emergency, urgent, and elective. Emergency procedures are done for life-threatening complications of fulminant colitis unresponsive to medical treatment. Urgent surgery is indicated in patients with severe ulcerative colitis who do not respond to inpatient intensive medical treatment. Failure or intolerance to long-term maintenance treatments and dysplasia or colorectal cancer are the main indications for elective procedures. Because the aim of emergency and urgent surgery is to restore patient health, the procedure involves removal of the inflamed colon via subtotal colectomy with a temporary ileostomy with no removal of the rectal stump. A pouch is typically avoided in this circumstance because of a high risk of pelvic bleeding, sepsis, and injury to pelvic nerves. After recovery, construction of an ileal pouch anal anastomosis (IPAA) and ileostomy closure can be done with a reduced risk of complications. Total proctocolectomy with IPAA is the standard of care for elective surgery (Fig. 23.1).
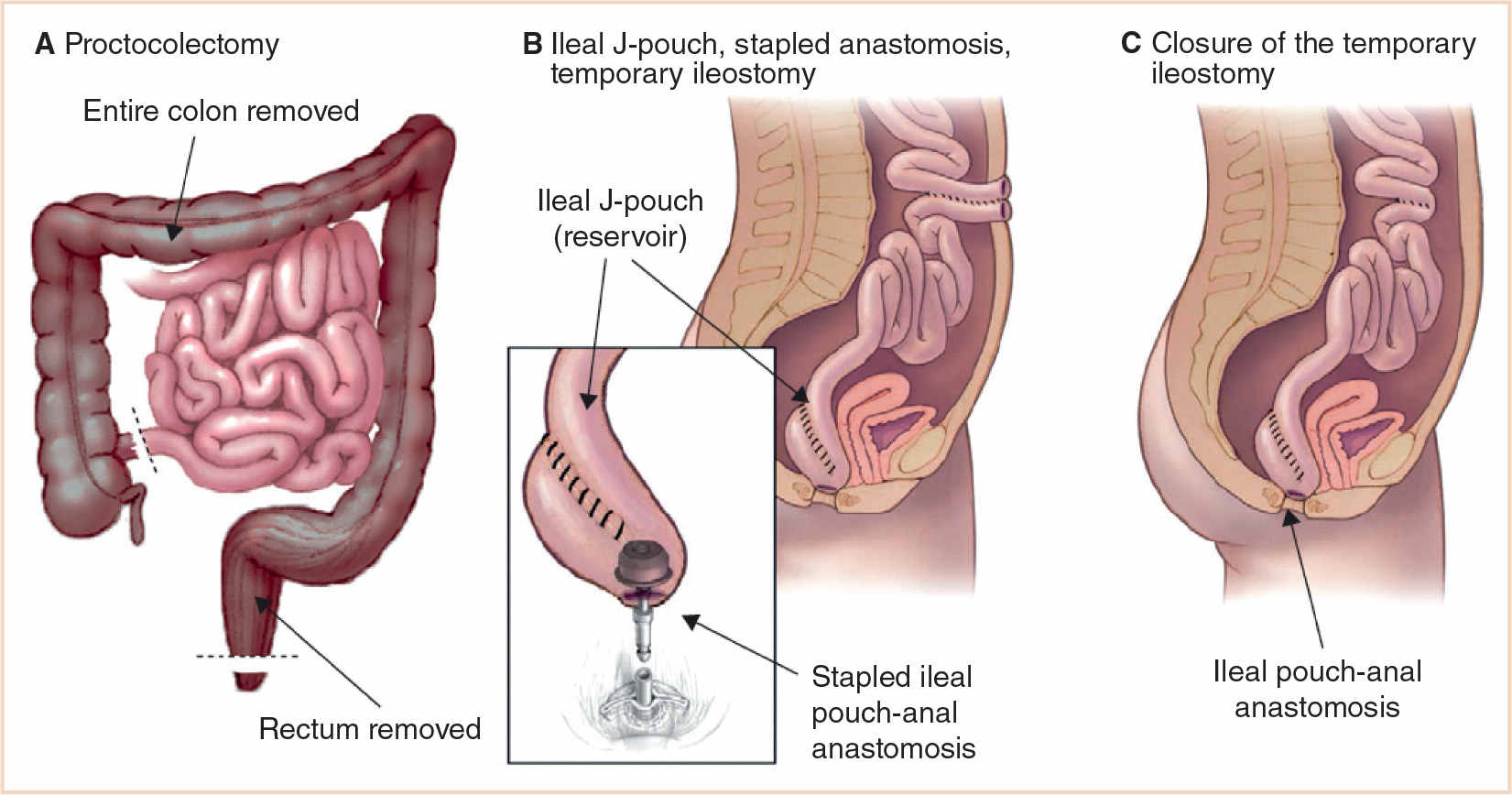
FIGURE 23.1 (A) Proctocolectomy. (B) Ileal J-pouch, stapled anastomosis, and temporary ileostomy. (C) Closure of the temporary ileostomy. The entire surgical procedure is based on four steps: removal of the colon; pelvic dissection and rectum removal sparing the pelvic nerves and the anal sphincter; construction of the ileal pouch, usually with the last 30–40 cm of the terminal ileum; and anastomosis of the pouch to the canal anal (From Ordás I, Eckmann L, Talamini M, et al. Ulcerative colitis. Lancet. 2012;380:1606–1619).
CROHN DISEASE
Unlike ulcerative colitis, surgery does not cure Crohn disease, and surgical treatment is directed to the relief of obstruction with removal of as little bowel as possible. Strictureplasty (Fig. 23.2) may be chosen over resection (6).Colon diversion or colectomy with ileostomy may be useful for severe perianal disease. Repeated bowel resection may lead to short bowel syndrome, and resection of terminal ileum to bile acid malabsorption with diarrhea and vitamin B12 malabsorption.
Because medical management is the principal treatment for Crohn disease, anesthetic plans have to account for concurrent drug therapy, as outlined above.
Prognostication for Crohn disease remains an evolving process; the recently introduced Lemann Score helps quantify the severity of disease (7). Young age, immediate need for corticosteroids, perianal disease, colonic resection, repeated small-bowel resection, a stricturing phenotype, substantial weight loss, and specific endoscopic lesions might predict a disabling disease course (Fig. 23.3).
ANESTHESIA ISSUES
READINESS FOR SURGERY
1. Airway management considerations may include full stomach/GI obstruction.
2. Preoperative laboratory tests are determined by the pertinent history.
3. Bowel prep preoperatively may be extensive.
ANESTHESIA GOALS
1. Avoidance of nitrous oxide (bowel distension) for prolonged surgery
2. Preservation of intraoperative temperature
3. Perioperative pain control
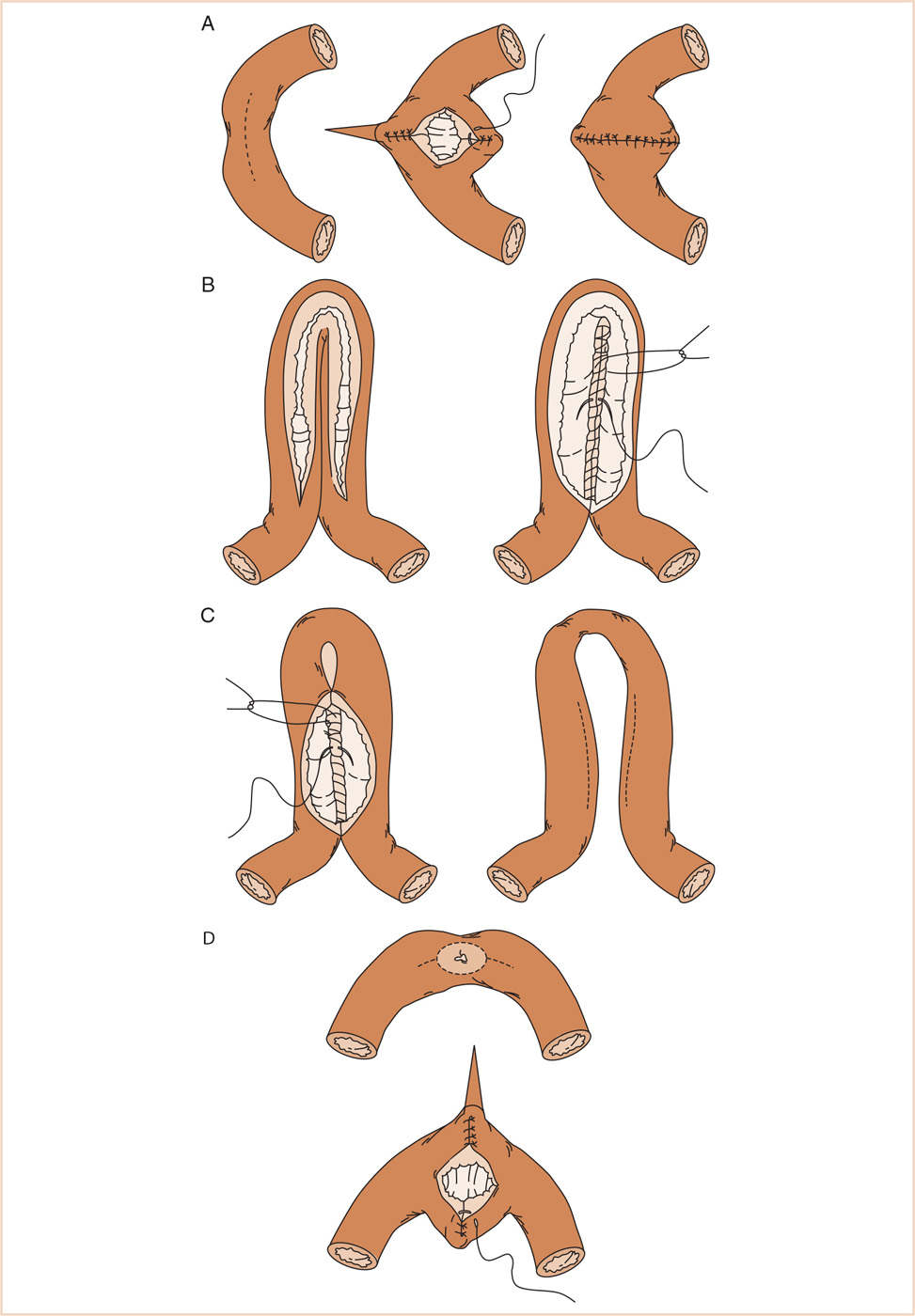
FIGURE 23.2 Various strictureplasty techniques for Crohn’s Disease. (A) Heineke–Mikulicz strictureplasty is performed by opening the small bowel along the antimesenteric border of the stricture and then closing it transversely. (B) Finney strictureplasty. After folding the strictured area onto itself, the enterotomy is made over the stenosis and the opposed surfaces of the bowel sutured together. (C) Jaboulay strictureplasty, a side-to-side enteroenterostomy. (D) Judd strictureplasty, with resection of the fistula site and closure of the enterotomy transversely, similar to the Heineke-Mikulicz technique (From Tichansky D, Cagir B, Yoo E, et al. Strictureplasty for Crohn’s disease: meta-analysis. Dis Colon Rectum. 2000;43:911–919).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


