(1)
Aschaffenburg, Germany
4.1 Introduction
The region of the shoulder joint is a preferred localisation of diverse causes of pain. These concerns not only solely local but also further proximal and sometimes also distally situated pathological changes in the shape of irritation and compression of the brachial plexus including its origins from C4-Th 1 and peripheral nerves.
In the first case, apart from arthrotic and arthritic as well as rheumatic changes of the shoulder and acromioclavicular joint, mainly diseases of the rotator cuff, summarised under the term humeroscapular periarthritis, are found. This includes affections of the subacromial, the subdeltoid and the subcoracoid bursa, as well as the adhesive capsulitis, called “frozen shoulder”. Up to now, the so-called coracoiditis was included as well, supposing this pathology is also a tendinopathy. This is not the case, however, as this localisation of pain mainly occurs in foraminal stenosis (C4-C7), thoracic outlet syndrome (TOS) and CRPS I, being treated by conservative or surgical therapy of these syndromes.
In the second case, it is pain radiation caused by proximal compression of the plexus roots mentioned (foramen stenosis) and the brachial plexus at the thoracic outlet (TOS and Sudeck’s dystrophy), whereas distal pressure damage occurs at the three main nerve trunks. The carpal tunnel syndrome is an example, known for long. In individual cases, some patients mainly complain about pain of the neck and discomfort radiating into the frontal upper shoulder region. These reactions can also be provoked by palpatory examination of the median nerve at the rascetta. The anterior thoracic nerve together with an articular branch of the stellate ganglion serves for pain projection, as they arise from the same cervical segments (C6-C8) as the median nerve. Similar reactions can also be triggered by a compression of the deep radial branch at the supinator gap, also possibly causing pain radiation into the lateral epicondyle area (TE) and the extension side of the wrist (neuralgia of the posterior interosseous nerve; Wachsmuth and Wilhelm 1967). A corresponding compression of the ulnar nerve at the ulnar nerve sulcus caused pain in extreme flexion and by the so-called flexion test (Wachsmuth and Wilhelm 1967). Further, local causes of pain apart from acute and chronic injury of the shoulder region and relatively rare pressure damage of the suprascapular nerve are internal diseases such as hyperuricaemia and pseudogout. Distant causes of pain such as Paget-von Schroetter syndrome, pulmonary tuberculosis, apoplectic insult and primarily myocardial infarction only lead to pain projection into the shoulder area and the arm. Distant pain can also be caused by subphrenic abscess and gall bladder, pancreatic and gastroduodenal diseases.
As diagnostic possibilities as well as conservative and surgical treatment of local causes of shoulder pain nowadays are excellent and successful, extensive denervation is not necessary in these cases. Thus, the denervation method by Nyakas and Kiss (1955) cutting only the posterior caudal articular nerve of the suprascapular and the axillar nerve in combination of an incision of the axillar recessus is only of historic interest.
On the contrary, in resistant severe pain radiation into the coracoid region, the shoulder and the AC joint, a partial denervation can be recommended. This is also true for the temporary pain elimination by blocking the entire shoulder innervation.
4.2 Surgically Relevant Anatomy and Physiology
A short synopsis concerning the shoulder innervation will be given; as in many relevant textbooks and atlases, a presentation of the articular nerves at the upper extremity is still missing. For more detailed information, I refer to the monograph by Rüdinger (1857) and the works of Gardner (1948) and see Ref. Wilhelm (1958, 1963, 1972), as well as to presentations of von Lanz and Wachsmuth (1959) and by Braus and Elze (1960).
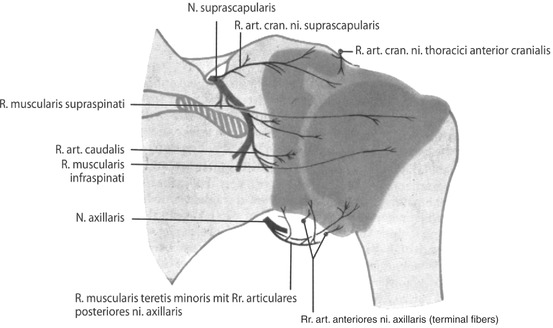
Branches of the suprascapular nerve innervate the extension side of the shoulder joint (Fig. 4.1). The upper, middle and lower articular nerves innervate the scapulohumeral joint capsule extramuscularly. The cranial articular branch of the suprascapular nerve also innervates the back side of the coracoid, finally reaching the acromioclavicular joint (AC joint). Intramuscularly, two further articular nerves come from the muscular branch of the supraspinatus and infraspinatus nerve, reaching the articular capsule at the insertion area of the muscles mentioned before. Caudally, the articular branches of the axillar nerve and the ramifications of its anterior articular branches follow at the lateral axillar hiatus.
The shoulder joint is innervated on the flexion side by intramuscular articular nerves in a deep layer, coming from 4 muscular branches of the subscapular nerves (Fig. 4.2). The most cranial branch also innervates the subcoracoid bursa; the remaining muscular branches end as articular fibres. The axillar recessus caudally is innervated by articular fibres of the axillar nerve before it enters the axillar gap. The most lateral articular fibres innervate the humeral capsule and the lesser tuberosity of the humerus. Figure 4.2 also shows a strikingly long subdeltoidal intertubercular branch of the axillar nerve, not only innervating the AC joint but also the major tuberosity of the humerus (Figs. 4.2 and 4.3).
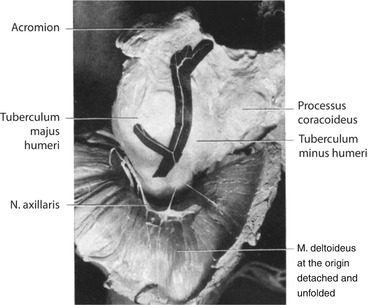
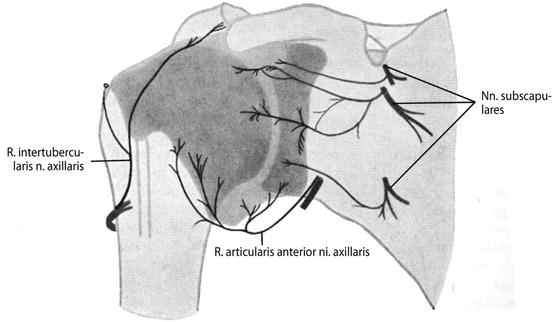
Fig. 4.3
Anatomic specimen: atypical course of the axillar nerve intertubercular branch, also innervating the AC joint. (From Wilhelm 1963)
An acromioclavicular articular branch is found in cranial direction in the superficial layer (Fig. 4.4), that is, in the extramuscular site, branching from the cranial anterior thoracic nerve. It runs over the coracoid process laterally, innervating it at its front and upper side and finally innervating the subacromial bursa and the AC joint. Shortly before the anterior cranial thoracic nerve enters the major pectoral muscle, a stronger nerve branch develops, running directly below the coracoid to the front rim of the deltoid muscle then branching below this muscle as variety of an intertubercular branch of the axillar nerve at the intertubercular synovial vagina (Fig. 4.4). This is normally innervated by a quite short branch of the axillar nerve up to the articular capsule (Fig. 4.5).
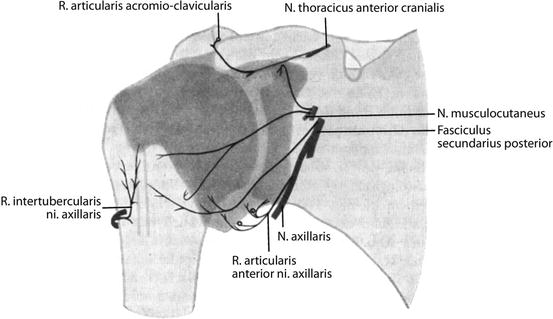
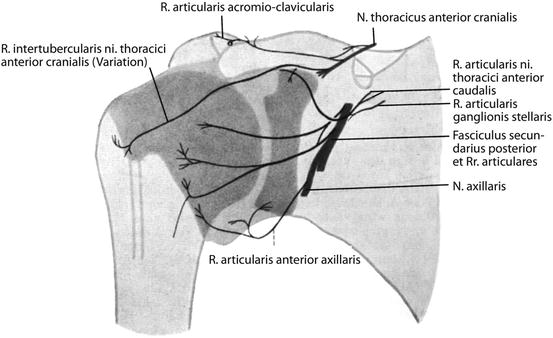
Fig. 4.5
Anterior innervation of the shoulder joint with regular course of axillar nerve intertubercular branch. (From Wilhelm 1972)
A branch of the caudal anterior thoracic nerve (Fig.4.4) or the musculocutaneous nerve (Fig. 4.5) innervates the subcoracoidal capsule section. Sympathetic fibres run together with this articular branch, coming from the cranial pole of the stellate ganglion, running to the back side of the subclavian artery and continuing distally in the adventitia of this vessel, permanently providing delicate fibres. One of them runs to the origin of the thoracoacromial artery from the axillar artery, finally connecting here with the articular branch of the caudal anterior thoracic nerve. Both structures run below the lateral fascicle of the brachial plexus and then move on to the front area of the subscapular muscle together with a small capsule vessel of the thoracoacromial artery towards the coracoid. Underneath, nerves and vessels enter the scapular capsule and the subcoracoid bursa, where a fine nerve strand also innervates the lower side of the coracoid and the coracoacromial ligament (Fig. 4.4).
In further distal direction, two articular branches arise from the posterior fascicle, running in a slight bow over the subscapular muscle towards the minor humeral tuberculum. The lowest branch can take over a part of the axillar nerve innervation area shown in Fig. 4.2, also originating from the posterior fascicle.
4.3 Epidemiology
Pain at the anterior upper quadrant of the shoulder joint region is not rare. Basically, these complaints are caused by a so-called coracoiditis. These testimonials, however, do not suffice for an objective, statistical evaluation of the incidence rate. There is an indirect possibility in examining the patient population of TOS and SD. A so-called coracoiditis develops in 71 % of 100 TOS patients surgically treated. In Sudeck’s dystrophy, the improvement rate accounts to 70 % of 20 patients; cf. postoperative results (Tables 5.10 and 5.11).
In so-called coracoiditis, we consequently have a projection of pain, just as in “epicondylitis”.
4.4 Etiology and Pathogenesis
As already mentioned initially (cf. Sect. 4.1), partial denervation is mainly useful in treatment of resistant severe pain radiation into the coracoid and acromial region (Table 4.1), basically being accomplished via the acromioclavicular articular branch of the cranial anterior thoracic nerve and articular branches of the stellate ganglion in connection with a branch of the caudal anterior thoracic nerve (Fig. 4.4).
Table 4.1
Thoracic outlet syndrome (1982–1987): findings at the shoulder girdle
Preoperative findings | Postoperative results | ||||
|---|---|---|---|---|---|
N p = 92 – follow-up – N op = 100 | Excellent | Good | Fair | Unchanged | |
Occipital pain | 28 → | 18 | 2 | 3 | 5 |
Upper cervical syndrome | 44 → | 28 | 4 | 6 | 6 |
Lower cervical syndrome | 72 → | 50 | 4 | 10 | 8 |
Trapezius muscle | 83 → | 49 | 7 | 15 | 12 |
Brachial plexus | 92 → | 64 | 10 | 7 | 11 |
Supraspinous fossa | 34 → | 22 | 1 | 7 | 4 |
Infraspinous fossa | 31 → | 19 | 2 | 7 | 3 |
Accessory nerve | 22 → | 8 | 1 | 7 | 6 |
Coracoid process | 71 → | 46 | 7 | 8 | 10 |
Acromion | 31 → | 13 | 4 | 8 | 6 |
Greater tuberosity of the humerus | 29 → | 16 | 1 | 4 | 8 |
Deltoid insertion | 48 → | 37 | 4 | 4 | 3 |
Total | 585 = 100 % | 370 = 63.3 % | 47 = 8 % | 86 = 14.7 % | 82 = 14 % |
Pain demanding surgical treatment is based on foramen stenosis, the therapy of which is not discussed here, and especially TOS and the difficultly distinguishable early manifestations of this syndrome, also Sudeck’s dystrophy (CRPS I), with a symptom complex showing striking parallels to TOS.
Pain at the AC joint and the acromion is mainly caused by arthrotic and arthritic processes, by subacromial impingement syndrome, injury of the rotator cuff and by calcificating tendinosis as well as by negative surgical results (Idelberger 1982, Tackmann et al. 1989, Wiedemann et al. 2007).
Shoulder pain requiring elimination in pre- and postoperative treatment is mainly caused by primary shoulder stiffness, also called adhesive capsulitis or frozen shoulder, resulting in a secondary shoulder stiffness, seen postoperatively after injury and surgery of the shoulder-arm region. The so-called periarthritic attack is a further essential cause of pain, occurring in tendinosis calcarea, being diagnosed by limited areas of calcification at the rotator cuff with corresponding osteoporotic changes at the greater tuberosity of the humerus.
4.5 Diagnostics
Besides pain at the shoulder joint, patients anamnestically frequently complain of pain at the back of the head and the neck muscles and of pain upon motion of the shoulder and the head (Table 4.1). Also, rest pain is reported, increasing at night in contrast to motion pain of the shoulder, due to an intense traction stress of nerve roots by a decrease of muscle tone with segmental character of pain radiation.
Myokinetic impairment is found upon examination of characteristic muscles (C5: deltoid muscle, C6: biceps muscle, C7: triceps muscle), as well as in decrease of crude strength.
The shoulder joint is mainly innervated by articular branches of the suprascapular nerves (C4-C6), the subscapular nerves (C5–/C7), the anterior thoracic nerves (C5-C8) and the axillar nerves (C5, C6).
A segmental examination is performed in order to exactly localise painful inhibitions of motion at the cervical spine; the behaviour of pain is checked in extension (improvement) and compression of the cervical spine (deterioration). X-rays of the cervical spine in two levels and in semi-diagonal position suffice for showing posttraumatic and degenerative articular changes, as well as stenoses of the intervertebral foramina. In ongoing segmental complaints, a CT or NMR should be performed immediately to rule out a luxation of an intervertebral disk, a tumour or an infectious/destructive process; a neurological examination then is necessary as well.
In the diagnosis of TOS, it primarily is most important to keep this syndrome in mind (Dunant 1975), especially since most of the patients already present with characteristic stress- and situation-connected complaints. Inspection should focus on an upward displacement of the scapula, relaxing the nerve-vessel strand in a cervical rib, as well as a shoulder girdle pushed forward, also relaxing the nerve-vessel bundle (Stöhr 2006).
An increase in diameter at the arm and hand together with an enlargement of the mamma at the same side, a pronounced venous pattern on the back of the hand and a visible collateral circle at the shoulder and chest are very important, possibly showing a venous impairment of the subclavian vein due to stenosis and congenital or acquired obstructions (“non-thrombotic occlusion” and Paget-von Schroetter syndrome).
The colour of the skin, temperature and trophics of the hand are important. Irritations of the brachial plexus at the upper thoracic outlet sometimes can lead to a Raynaud phenomenon or frequently to a Horner syndrome. In atrophy of the inner hand muscles, a pressure damage of the lower plexus roots (C8 and Th1) is possible. Pulse control in hanging arm and pressure stress of the shoulder girdle, as well as diverse provocation tests, like the carrying test (anamnesis), the abduction test (3-min fist-closure test) according to Roos (1979) and the elevation test, give first hints at an involvement of the vascular system, whereas redressment of the shoulder girdle can result in irritation of the lower plexus roots with radiation of pain into the area of the hand and the fingers.
Related posts:
 The Controversial Pain Syndrome of Proximal Radial Compression Syndrome (PRKS): Pathogenesis and Surgical Treatment of Resistant Cases
The Controversial Pain Syndrome of Proximal Radial Compression Syndrome (PRKS): Pathogenesis and Surgical Treatment of Resistant Cases
 The Controversial Pain Syndrome of GE: Pathogenesis and Surgical Treatment of Resistant Cases
The Controversial Pain Syndrome of GE: Pathogenesis and Surgical Treatment of Resistant Cases
 The Controversial Pain Syndrome of Tennis Elbow (TE): Pathogenesis and Surgical Treatment of Resistant Cases
The Controversial Pain Syndrome of Tennis Elbow (TE): Pathogenesis and Surgical Treatment of Resistant Cases
 Controversial Pain Syndrome of M. Sudeck (RSD, CRPS I): Pathogenesis and Surgical Treatment of Resistant Cases
Controversial Pain Syndrome of M. Sudeck (RSD, CRPS I): Pathogenesis and Surgical Treatment of Resistant Cases
 Physical Examination of the Patient With Pain
Physical Examination of the Patient With Pain
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


