The Basal Infusion Mode in Patient-controlled Analgesia Is Both Friend and Foe
Amit Sharma MD
Patient-controlled analgesia (PCA) is the core therapeutic drug delivery system in acute and acute-on-chronic pain settings. Historically, in 1971, Sechzer published the first report showing the safety and efficacy of delivering small incremental doses of opioids using a machine. Since his initial description, this novel technique of analgesic drug delivery has been enormously refined and widely accepted. It emanated from the basic pharmacologic principle that a given analgesic medication needs to attain a specific serum concentration to produce analgesia. The lowest drug levels at which this is accomplished is the minimum effective analgesic concentration (MEAC) of that particular drug. Maintaining a constant serum drug concentration above MEAC would thus result in sustained analgesia. It is almost impossible to achieve stable serum drug levels with intermittent oral and intramuscular drug delivery methods. They often result in peaks of high drug concentrations that cause side effects and troughs of lower drug levels leading to inadequate analgesia (Fig. 166.1). These variations in drug levels can be avoided with the use of intermittent small intravenous (IV) doses or a continuous infusion.
Using these principles, opioids are now often delivered intravenously using highly sophisticated microprocessor-controlled units (e.g., PCA machine) in numerous acute and certain selected chronic pain settings. These machines allow several modes of drug administration, some of which are as follows:
Demand-Only Mode (DOM): This is the most commonly used method. The patient can self-administer a fixed dose (demand dose) into their IV.
Continuous Plus Demand Mode (CDM): A fixed baseline (basal or background) dose is infused intravenously every hour in addition to demand dosing.
Variable-Rate Infusion Plus Demand Mode (VID): In addition to patient dosing, continuous basal rate is preprogrammed on an internal clock to vary, turn on, or turn off during specified hours of the day.
Variable-Rate Feedback Infusion Plus Demand Mode (VFID): Basal infusion rate is varied by the PCA machine’s microprocessor and is based on patient’s usage.
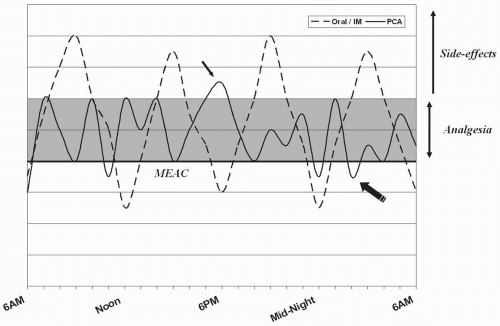 FIGURE 166.1. Comparison of systemic drug concentrations (y axis) during conventional oral or intramuscular (IM) opioid drug delivery system and during patient-controlled analgesia (PCA) use. The dark line demonstrates the minimally effective analgesic concentration (MEAC), and the shaded area represents the analgesic window. Serum drug concentrations above the analgesic window (thin arrow) result in clinically relevant side effects, while those below (bold arrow) cause poor pain control. |
Given the widespread use of PCA in postoperative settings, it is imperative for all anesthesiologists to have a precise understanding of their functioning. Although standard PCA guidelines exist for postoperative analgesia (Table 164.3), confusion often prevails with regard to basal infusion. Proponents of basal infusion claim that it allows better patient satisfaction because the demand frequency with CDM is lower than in DOM. It seems that the constant IV infusion of opioid would maintain a certain level of serum drug levels and would then be easier to reach the MEAC using fewer demand doses (Fig. 166.2). In reality, this perception is oversimplistic and does not account for multiple variables on which drug pharmacokinetics actually depends. For instance, the serum drug concentration required to reach MEAC varies from one individual to the next. This situation is further complicated by the fact that significant interpersonal variability exists for the safe analgesic window, which is defined as the serum drug concentrations that are associated with clinically relevant analgesia without any side effects (shaded area in Fig. 166.1). Certain individuals, such as elderly people, have relatively narrow analgesic windows, and use of basal infusion would pose undue risks for side effects in these patients.
The futility and risks of basal infusion, especially in opioid-naïve patients, has been shown in multiple studies (Table 166.1). Guler et al. showed significant improvement in pain scores with the use of CDM technique in the postoperative pain setting, but most other studies have failed to replicate those results. Even with similar analgesic response, opioid consumption has been shown to be higher with CDM than with DOM in numerous studies. Moreover, the low-dose continuous nighttime-only infusion (VID mode) failed to show any improvement in patients’ sleep or comfort in most studies (Table 166.1). CDM technique in these studies failed to show any major increase in the incidence of severe side effects. Other studies and case series, in contrast, have frequently linked the additional background opioid infusion to myriad side effects. Some of the feared complications include respiratory depression and higher chances of programming errors.
Related posts:
 Never Neglect the Basics of Airway Management
Consider the Use of Lidocaine in the Cuff of the Endotracheal Tube, But Be Aware of the Risks and Alternatives
Do Not Underestimate the Difficulty of Reintubating a Patient Who Has Undergone Carotid Endarterectomy or Cervical Spine Surgery
Don’t Overflush Lines
Do Not Treat Lactic Acidosis with Bicarbonate
Beware the Antibiotic Bowel Prep
Never Neglect the Basics of Airway Management
Consider the Use of Lidocaine in the Cuff of the Endotracheal Tube, But Be Aware of the Risks and Alternatives
Do Not Underestimate the Difficulty of Reintubating a Patient Who Has Undergone Carotid Endarterectomy or Cervical Spine Surgery
Don’t Overflush Lines
Do Not Treat Lactic Acidosis with Bicarbonate
Beware the Antibiotic Bowel Prep
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


