Study objective
Palliative care has been shown to reduce end-of-life emergency department (ED) use. Our objective was to determine how the association of community-based palliative care with reduced ED visits in the last year of life varied by patient factors.
Methods
This was a retrospective cohort study of 11,875 decedents who died with neoplasms, heart failure, renal failure, chronic obstructive pulmonary disease, or liver failure in Western Australia in 2009 to 2010. Outcome measures were adjusted hazard ratios (HRs) and daily (hazard) rates of ED visits.
Results
The adjusted average rate of ED visits for the cohort was reduced 50% (HR 0.50; 95% confidence interval [CI] 0.47 to 0.53) during periods of receipt of community-based palliative care. This relative reduction in ED visits varied by patient factors, ranging from 43% (HR 0.57; 95% CI 0.45 to 0.74) for decedents aged 60 years and younger up to 71% (HR 0.29; 95% CI 0.18 to 0.46) for people aged 90 years and older. Decedents living in the most disadvantaged areas had a 44% (HR 0.56; 95% CI 0.44 to 0.72) reduction in ED visits when receiving community-based palliative care compared with a 60% (HR 0.40; 95% CI 0.31 to 0.53) reduction for decedents who lived in the least disadvantaged areas and received this care. The ED visit rates while patients were receiving palliative care also varied by ED visit history, partner status, and region of residence.
Conclusion
Receipt of community-based palliative care in the last year of life was associated with a reduced rate of ED visits. The magnitude of this association was modified by patient health, as well as social and demographic factors.
Introduction
Emergency department (ED) use increases significantly toward the end of life. Numerous studies have reported that community (home)-based palliative care for people with life-limiting conditions is associated with reduced use of acute care health services. Although multidisciplinary palliative care has been demonstrated to reduce acute care service use, not all use of the ED is unwarranted. A study of cancer patients receiving outpatient palliative care in the United States reported that 77% of ED visits were unavoidable. However, even if most ED visits of cancer patients in the last 2 weeks of life result in hospital admission, it does not necessarily mean that the patient could have been managed only in the acute care setting. Ideally, high-quality palliative care should be able to manage the most common acute symptoms of the dying person without hospitalization.
What is already known on this topic
Palliative care reduces emergency department (ED) use near the end of life.
What question this study addressed
This study examined ED use during the final year of life among 11,875 patients in Western Australia, of whom 32% received at least some palliative care. The effect of palliative care on ED use among patient subgroups is examined.
What this study adds to our knowledge
Overall, patients receiving community-based palliative care were less likely to seek ED care. The reduction in ED visits associated with palliative care was greater for older patients, patients living in higher socioeconomic status areas, and those with fewer previous ED visits.
How this is relevant to clinical practice
These observational findings suggest that the influence of palliative care on ED use at the end of life is not uniform.
Historically, palliative care evolved to meet the end-of-life needs of cancer patients. It has since become apparent that it benefits noncancer terminal conditions such as renal failure, heart failure, chronic obstructive pulmonary disease, and liver failure, although access to and quality of palliative care for these conditions could be improved. In Australia, there has been evidence of this improved access to palliative care in noncancer conditions during the last 10 years.
The objective of this study was to describe patterns of use of EDs by people in their last year of life and how this varied when they received community-based palliative care. We also investigated whether any patient health, social, and demographic factors modified the rates of ED visits while patients were receiving community-based palliative care.
Materials and Methods
Study Design
This was a retrospective cohort study of persons aged 20 years and older who died from medical conditions considered amenable to palliative care. A linked deidentified extraction of all hospital admission records, death records, hospital ED visits, and community-based care records was obtained from the Data Linkage Branch, Western Australian Department of Health. The ED presentations from 365 days before the date of death until death (ie, the last year of life), as well as place of residence at each hospital admission and at death, were available for each decedent. Ethical approval was obtained from Curtin University and the Western Australian Department of Health Human Research Ethics Committees.
The final cohort was selected from death registration records. People who died with conditions amenable to palliative care in Western Australia from January 1, 2009, to December 31, 2010, and who were aged 20 years or older were identified. This was achieved by searching part 1 of the death certificate (underlying causes of death) for any mention of the most frequent conditions amenable to palliative care identified by Rosenwax et al, namely, neoplasia, heart failure, renal failure, liver failure, chronic obstructive pulmonary disease, Alzheimer’s disease, motor neuron disease, Parkinson’s disease, Huntington’s disease, and HIV/AIDS. The underlying antecedent cause of death took precedence over more direct causes of death when more than one condition amenable to palliative care was present. Because of small sample sizes, decedents with motor neuron disease, Parkinson’s disease, Huntington’s disease, and HIV/AIDS were excluded. Decedents with Alzheimer’s dementia were also excluded because we have published a detailed analysis of ED use and palliative care in this group elsewhere.
Community-based palliative care was defined as the palliative care provided by the nonprofit organization Silver Chain Western Australia, which provides more than 90% of in-home palliative care in Western Australia. Their community-based palliative care service area is largely based in the major metropolitan city of Perth, where approximately 75% of the state population resides. The community-based palliative care service is 24-hour in-home specialist nursing and, where required, medical service provided by primary care physicians and palliative care specialists. Care includes at-home physical care and practical support, symptom management (for example, pain and nausea), counseling, a respite option, and links to other community, spiritual, and government services. Silver Chain also provide a palliative nurse consultancy service to public and private hospitals and residential care facilities where patient care is managed by a registered nurse 24 hours a day. A palliative rural telephone advisory service offers specialist advice and knowledge to rural service providers in regard to the palliative care needs of specific patients.
Access to community-based palliative care requires referral from a medical practitioner or hospital for patients with active, progressive, terminal illness requiring symptom management. This generally occurs within 3 months of death but can be 12 months or more from death. It has been reported that patients with life-limiting conditions with slow or fluctuating trajectories that required longer-term palliative care may have more difficulty accessing it.
An ED visit was defined as the first presentation of the day to an ED whether it resulted in a hospital admission or not. Multiple presentations to the ED on the same day were considered a single ED visit. The ED visits that occurred as part of hospital transfers were excluded from the analysis. Available ED data included the triage category, hospital admission status, and presenting symptom. Coded presenting symptom information was available for major metropolitan public hospitals only (approximately 80% of ED visits). The number of previous ED visits that had already occurred in the last year of life at each ED visit was recorded.
Residential address was classified as private residence, residential aged care facility, other types of care facilities, or other/unknown. Marital status at death was classified as partnered or nonpartnered. Accessibility categories were based on the Accessibility/Remoteness Index of Australia (ARIA+) index, which measures accessibility to services by taking road distances to nearest service centers and population size into account. Socioeconomic status was estimated from the Index of Relative Social Disadvantage, which estimates the average social disadvantage of small geographic areas according to 17 measures, including education, income, occupation, and unemployment. Comorbidity was defined as the presence of 1 or more of the 30 Elixhauser conditions recorded during inpatient hospital stays after exclusion of the principal condition leading to death.
Primary Data Analysis
χ 2 Tests were used to assess the equality of proportions. Linear regression models were used to assess equality of means across principal conditions, using neoplasia as the reference groups. Nonparametric K-sample tests for the equality of medians were used.
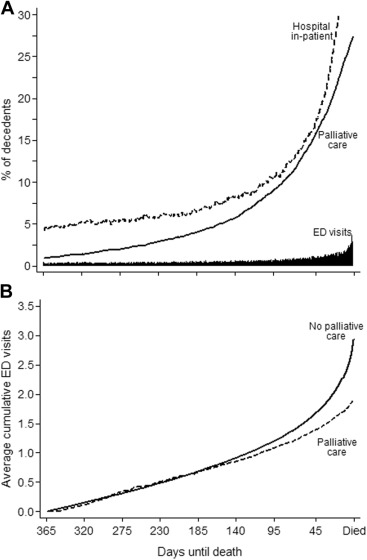
For the time-to-event (survival) analyses, a marginal-models approach was used and multiple ED visits per decedent were accounted for with robust variance estimators. Each day in the last year of life of each decedent was assigned as no care (no hospital- or community-based palliative care), inpatient hospital care, or community-based palliative care.
A decedent was not considered at risk of an ED admission while in the hospital, and his or her data were removed from the risk pool during each hospital stay (interval truncation). The Nelson-Aalen estimator of the cumulative hazard function was used to visualize the accumulated total average number of ED visits in the last year of life. Because decedents could switch between receiving palliative care and then not receiving it, the Figure does not necessarily represent the same group of decedents on any one day.
To easily visualize the baseline hazards, a flexible parametric proportional hazards model that used restricted cubic splines (Royston-Parmar models) was constructed. Time-fixed (eg, sex) and time-varying covariates (eg, ED history and community-based palliative care state) variables were included. Time-dependent effects, ie, when the hazard ratio of a covariate changed over time (nonproportional hazards), were modeled as cubic splines. Interaction terms were included in the final model if the joint test of the 2 interaction terms or the test of an interesting partial interaction effect resulted in P <.05. Baseline complexity was described with 7 internal knots for the main model and 2 for the time-dependent effects. Stata (version 13; StataCorp, College Station, TX) was used.
Materials and Methods
Study Design
This was a retrospective cohort study of persons aged 20 years and older who died from medical conditions considered amenable to palliative care. A linked deidentified extraction of all hospital admission records, death records, hospital ED visits, and community-based care records was obtained from the Data Linkage Branch, Western Australian Department of Health. The ED presentations from 365 days before the date of death until death (ie, the last year of life), as well as place of residence at each hospital admission and at death, were available for each decedent. Ethical approval was obtained from Curtin University and the Western Australian Department of Health Human Research Ethics Committees.
The final cohort was selected from death registration records. People who died with conditions amenable to palliative care in Western Australia from January 1, 2009, to December 31, 2010, and who were aged 20 years or older were identified. This was achieved by searching part 1 of the death certificate (underlying causes of death) for any mention of the most frequent conditions amenable to palliative care identified by Rosenwax et al, namely, neoplasia, heart failure, renal failure, liver failure, chronic obstructive pulmonary disease, Alzheimer’s disease, motor neuron disease, Parkinson’s disease, Huntington’s disease, and HIV/AIDS. The underlying antecedent cause of death took precedence over more direct causes of death when more than one condition amenable to palliative care was present. Because of small sample sizes, decedents with motor neuron disease, Parkinson’s disease, Huntington’s disease, and HIV/AIDS were excluded. Decedents with Alzheimer’s dementia were also excluded because we have published a detailed analysis of ED use and palliative care in this group elsewhere.
Community-based palliative care was defined as the palliative care provided by the nonprofit organization Silver Chain Western Australia, which provides more than 90% of in-home palliative care in Western Australia. Their community-based palliative care service area is largely based in the major metropolitan city of Perth, where approximately 75% of the state population resides. The community-based palliative care service is 24-hour in-home specialist nursing and, where required, medical service provided by primary care physicians and palliative care specialists. Care includes at-home physical care and practical support, symptom management (for example, pain and nausea), counseling, a respite option, and links to other community, spiritual, and government services. Silver Chain also provide a palliative nurse consultancy service to public and private hospitals and residential care facilities where patient care is managed by a registered nurse 24 hours a day. A palliative rural telephone advisory service offers specialist advice and knowledge to rural service providers in regard to the palliative care needs of specific patients.
Access to community-based palliative care requires referral from a medical practitioner or hospital for patients with active, progressive, terminal illness requiring symptom management. This generally occurs within 3 months of death but can be 12 months or more from death. It has been reported that patients with life-limiting conditions with slow or fluctuating trajectories that required longer-term palliative care may have more difficulty accessing it.
An ED visit was defined as the first presentation of the day to an ED whether it resulted in a hospital admission or not. Multiple presentations to the ED on the same day were considered a single ED visit. The ED visits that occurred as part of hospital transfers were excluded from the analysis. Available ED data included the triage category, hospital admission status, and presenting symptom. Coded presenting symptom information was available for major metropolitan public hospitals only (approximately 80% of ED visits). The number of previous ED visits that had already occurred in the last year of life at each ED visit was recorded.
Residential address was classified as private residence, residential aged care facility, other types of care facilities, or other/unknown. Marital status at death was classified as partnered or nonpartnered. Accessibility categories were based on the Accessibility/Remoteness Index of Australia (ARIA+) index, which measures accessibility to services by taking road distances to nearest service centers and population size into account. Socioeconomic status was estimated from the Index of Relative Social Disadvantage, which estimates the average social disadvantage of small geographic areas according to 17 measures, including education, income, occupation, and unemployment. Comorbidity was defined as the presence of 1 or more of the 30 Elixhauser conditions recorded during inpatient hospital stays after exclusion of the principal condition leading to death.
Primary Data Analysis
χ 2 Tests were used to assess the equality of proportions. Linear regression models were used to assess equality of means across principal conditions, using neoplasia as the reference groups. Nonparametric K-sample tests for the equality of medians were used.
For the time-to-event (survival) analyses, a marginal-models approach was used and multiple ED visits per decedent were accounted for with robust variance estimators. Each day in the last year of life of each decedent was assigned as no care (no hospital- or community-based palliative care), inpatient hospital care, or community-based palliative care.
A decedent was not considered at risk of an ED admission while in the hospital, and his or her data were removed from the risk pool during each hospital stay (interval truncation). The Nelson-Aalen estimator of the cumulative hazard function was used to visualize the accumulated total average number of ED visits in the last year of life. Because decedents could switch between receiving palliative care and then not receiving it, the Figure does not necessarily represent the same group of decedents on any one day.
To easily visualize the baseline hazards, a flexible parametric proportional hazards model that used restricted cubic splines (Royston-Parmar models) was constructed. Time-fixed (eg, sex) and time-varying covariates (eg, ED history and community-based palliative care state) variables were included. Time-dependent effects, ie, when the hazard ratio of a covariate changed over time (nonproportional hazards), were modeled as cubic splines. Interaction terms were included in the final model if the joint test of the 2 interaction terms or the test of an interesting partial interaction effect resulted in P <.05. Baseline complexity was described with 7 internal knots for the main model and 2 for the time-dependent effects. Stata (version 13; StataCorp, College Station, TX) was used.
Results
There were 12,817 deaths in Western Australia from 1 or more of 10 conditions identified as being amenable to palliative care during the study period (2009 to 2010). Of these, 11,875 decedents (93%) had 1 or more of the 5 most frequent conditions amenable to palliative care, namely, neoplasm, heart failure, renal failure, chronic obstructive pulmonary disease, and liver failure. This group of decedents formed the cohort of interest. Most of the cohort (n=9,212; 78%) attended an ED at least once in the last year of life, resulting in a combined total of 26,020 ED visits. The median number of ED visits per decedent was 2 (interquartile range 1 to 4), although there was a wide range, with 1 decedent recording 74 ED visit days in the last year of life.
The social, demographic, and health characteristics of decedents varied significantly by the number of ED visits in the last year of life ( Table 1 ). The proportion of decedents who had 3 or more ED visits increased with younger age, remoteness, social disadvantage, and dying with liver failure. The proportion of decedents who did not visit an ED in the last year of life was greater for women, decedents with partners, and decedents dying from neoplasms. The presence of any one of the 30 Elixhauser comorbid conditions was associated with a greater proportion of ED visits compared with that for the cohort as a whole.
| Decedent Characteristics | Number of ED Visits During the Last Year of Life | |||||||
|---|---|---|---|---|---|---|---|---|
| None | 1 | 2 | ≥3 | |||||
| No. | % | No. | % | No. | % | No. | % | |
| Overall | 2,663 | 22.4 | 3,180 | 26.7 | 2,188 | 18.4 | 3,844 | 32.4 |
| Age at death, y | ||||||||
| <60 | 334 | 20.6 | 350 | 21.6 | 267 | 16.5 | 669 | 41.3 |
| 60–69 | 463 | 23.8 | 501 | 25.7 | 345 | 17.7 | 639 | 32.8 |
| 70–79 | 629 | 20.9 | 845 | 28.1 | 537 | 17.8 | 998 | 33.2 |
| 80–89 | 830 | 21.8 | 1,087 | 28.6 | 736 | 19.4 | 1,149 | 30.2 |
| ≥90 | 407 | 27.2 | 397 | 26.5 | 303 | 20.3 | 389 | 26.0 |
| Sex | ||||||||
| Male | 1,421 | 21.8 | 1,677 | 25.7 | 1,171 | 17.9 | 2,260 | 34.6 |
| Female | 1,242 | 23.2 | 1,503 | 28.1 | 1,017 | 19.0 | 1,584 | 29.6 |
| Partnered at death | ||||||||
| No | 1,333 | 21.1 | 1,758 | 27.8 | 1,185 | 18.8 | 2,037 | 32.3 |
| Yes | 1,330 | 23.9 | 1,422 | 25.6 | 1,003 | 18.0 | 1,807 | 32.5 |
| Accessibility index | ||||||||
| Major cities | 2,030 | 25.2 | 2,251 | 27.9 | 1,477 | 18.3 | 2,302 | 28.6 |
| Inner regional | 338 | 17.3 | 520 | 26.6 | 390 | 19.9 | 707 | 36.2 |
| Outer regional | 195 | 16.9 | 272 | 23.6 | 208 | 18.1 | 477 | 41.4 |
| Remote | 59 | 14.4 | 80 | 19.5 | 72 | 17.5 | 200 | 48.7 |
| Very remote | 29 | 13.1 | 37 | 16.7 | 27 | 12.2 | 129 | 58.1 |
| Unknown | — | — | 9 | 18.8 | 10 | 20.8 | 27 | 56.3 |
| Index of Relative Social Disadvantage | ||||||||
| Most disadvantaged | 394 | 15.2 | 633 | 24.4 | 499 | 19.2 | 1,072 | 41.3 |
| More disadvantaged | 477 | 18.5 | 685 | 26.6 | 521 | 20.2 | 897 | 34.8 |
| Average disadvantaged | 528 | 21.9 | 652 | 27.0 | 461 | 19.1 | 774 | 32.0 |
| Less disadvantaged | 495 | 24.7 | 561 | 28.0 | 355 | 17.7 | 590 | 29.5 |
| Least disadvantaged | 757 | 34.3 | 628 | 28.5 | 339 | 15.4 | 483 | 21.9 |
| Unknown | — | — | 9 | 19.6 | 9 | 19.6 | 26 | 56.5 |
| Residence at death | ||||||||
| Private | 2,122 | 22.3 | 2,518 | 26.5 | 1,749 | 18.4 | 3,121 | 32.8 |
| Residential aged care | 479 | 22.8 | 603 | 28.7 | 387 | 18.4 | 632 | 30.1 |
| Other care facility | 35 | 27.6 | 26 | 20.5 | 24 | 18.9 | 42 | 33.1 |
| Unknown/other/no fixed address | 23 | 39.7 | 11 | 19.0 | 7 | 12.1 | 17 | 29.3 |
| Principal condition underlying death | ||||||||
| Neoplasms | 1,840 | 24.8 | 1,981 | 26.7 | 1,384 | 18.7 | 2,206 | 29.8 |
| Heart failure | 395 | 19.6 | 560 | 27.7 | 378 | 18.7 | 686 | 34.0 |
| Renal failure | 205 | 17.9 | 285 | 24.9 | 227 | 19.8 | 428 | 37.4 |
| Chronic obstructive pulmonary disease | 202 | 18.5 | 296 | 27.1 | 177 | 16.2 | 419 | 38.3 |
| Liver failure | 21 | 10.2 | 58 | 28.2 | 22 | 10.7 | 105 | 51.0 |
| Elixhauser comorbid conditions ∗ | ||||||||
| Metastatic cancer | 33 | 15.4 | 55 | 25.7 | 41 | 19.2 | 85 | 39.7 |
| Rheumatoid arthritis/collagen vascular | 24 | 15.3 | 34 | 21.7 | 31 | 19.7 | 68 | 43.3 |
| Liver disease | 81 | 14.4 | 138 | 24.5 | 95 | 16.9 | 249 | 44.2 |
| Solid tumor without metastasis | 58 | 14.3 | 101 | 24.9 | 81 | 20.0 | 166 | 40.9 |
| Depression | 91 | 14.2 | 146 | 22.8 | 121 | 18.9 | 281 | 44.0 |
| Pulmonary circulation disorders | 118 | 12.8 | 211 | 23.0 | 179 | 19.5 | 411 | 44.7 |
| Paralysis | 73 | 11.8 | 158 | 25.6 | 136 | 22.0 | 250 | 40.5 |
| Renal failure | 178 | 11.7 | 343 | 22.6 | 301 | 19.9 | 693 | 45.7 |
| Coagulopathy | 159 | 11.7 | 308 | 22.6 | 255 | 18.7 | 640 | 47.0 |
| Peripheral vascular disorders | 100 | 11.7 | 203 | 23.8 | 155 | 18.2 | 394 | 46.2 |
| Other neurologic disorders | 107 | 11.4 | 209 | 22.2 | 198 | 21.1 | 426 | 45.3 |
| Cardiac arrhythmias | 341 | 11.3 | 769 | 25.5 | 617 | 20.4 | 1,291 | 42.8 |
| Fluid and electrolyte disorders | 478 | 10.7 | 1,083 | 24.3 | 888 | 19.9 | 2,003 | 45.0 |
| Diabetes, uncomplicated | 56 | 10.7 | 121 | 23.0 | 99 | 18.9 | 249 | 47.4 |
| Peptic ulcer disease excluding bleeding | 15 | 10.7 | 29 | 20.7 | 22 | 15.7 | 74 | 52.9 |
| Diabetes, complicated | 207 | 10.3 | 463 | 23.1 | 413 | 20.6 | 925 | 46.1 |
| Weight loss | 68 | 10.2 | 186 | 27.8 | 137 | 20.5 | 278 | 41.6 |
| Congestive heart failure | 152 | 9.8 | 357 | 23.0 | 298 | 19.2 | 743 | 47.9 |
| Psychoses | 7 | 9.7 | 15 | 20.8 | 15 | 20.8 | 35 | 48.6 |
| Drug abuse | 9 | 9.6 | 19 | 20.2 | 11 | 11.7 | 55 | 58.5 |
| Hypertension, uncomplicated | 334 | 9.4 | 875 | 24.5 | 734 | 20.6 | 1,628 | 45.6 |
| Valvular disease | 61 | 9.1 | 165 | 24.5 | 127 | 18.9 | 320 | 47.5 |
| Deficiency anemia | 52 | 8.9 | 128 | 21.9 | 106 | 18.1 | 299 | 51.1 |
| Chronic pulmonary disease | 105 | 8.7 | 262 | 21.7 | 261 | 21.6 | 580 | 48.0 |
| Hypertension, complicated | 13 | 8.6 | 31 | 20.4 | 32 | 21.1 | 76 | 50.0 |
| Hypothyroidism | 11 | 8.4 | 23 | 17.6 | 29 | 22.1 | 68 | 51.9 |
| Lymphoma | — | — | 12 | 24.5 | — | — | 26 | 53.1 |
| Blood loss anemia | 21 | 7.7 | 49 | 18.0 | 43 | 15.8 | 159 | 58.5 |
| Obesity | 17 | 6.4 | 58 | 21.9 | 48 | 18.1 | 142 | 53.6 |
| Alcohol abuse | 24 | 5.3 | 105 | 23.0 | 71 | 15.6 | 256 | 56.1 |
Related posts:
 Adolescent Male With Right Shoulder Pain After Football Injury
Adolescent Male With Right Shoulder Pain After Football Injury
 Association Between the Opening of Retail Clinics and Low-Acuity Emergency Department Visits
Bending the Curve of Health Trajectories for Older Adults Discharged From the Emergency Department
Yet Another
Sedating the Agitated Patient: A Moving Target?
Classified 2017 Advertising Rates & Information
Association Between the Opening of Retail Clinics and Low-Acuity Emergency Department Visits
Bending the Curve of Health Trajectories for Older Adults Discharged From the Emergency Department
Yet Another
Sedating the Agitated Patient: A Moving Target?
Classified 2017 Advertising Rates & Information
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


