12 Tendon Sheath and Insertion Injections
Tendons are impressively strong structures that link muscles to bone. They function to transmit the force of muscular contraction to a bone, thereby moving a joint or helping to immobilize a body part. Their microscopic organization is thoroughly described elsewhere.1–3
The organizational unit in a tendon is the collagen fibril, which collectively forms fascicles, which as a group compose the tendon itself.4 Some tendons, especially long ones, are guided and lubricated along their paths by sheaths (Fig. 12-1) (e.g., biceps brachii, (Fig. 12-2) extensor pollicis brevis, and abductor pollicis longus).
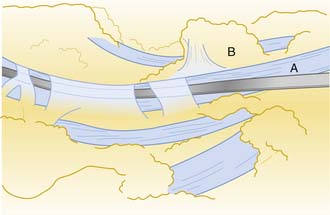
Figure 12-1 Drawing demonstrating a flexor tendon (A) within its sheath. The paratendinous septum is reflected (B).
A prototypical muscle consists of the muscle belly centrally, two musculotendinous junctions, and tendinous insertions into bone at the points of anatomic origin and insertion.5 Some muscles, such as the extensor carpi radialis longus and brevis at the elbow, attach directly into bone (Figs. 12-3), an arrangement that may be more susceptible to injury.6
Much is known about a tendon’s response to laceration and operative repair,2 although this clinical situation is not frequently encountered. Less is understood about the more common and clinically relevant overuse tendinitis. A tendon and its sheath (if present) will undergo a typical inflammatory response to acute or chronic overuse injury, followed by a regenerative repair process.2,7,8 The distinction between an overload type of acute injury and a chronic overuse mechanism will aid in successful rehabilitation of tendinitis.9
Corticosteroid Injections
Cortisone and its derivatives are known to reduce or prevent inflammation. Numerous corticosteroid preparations are available for local injection10 (see Chapter 2 on medications). The injectable corticosteroids are suspensions of insoluble particles, and therefore, the antiinflammatory effect is profound only where the material is deposited.11 The ability of corticosteroids to control inflammation makes them a valuable adjunct in treating tendon injuries because they do not alter the underlying process that leads to inflammation.10
Efficacy
McWhorter and colleagues injected hydrocortisone acetate into rat Achilles peritenons that had been previously injured.3 There were no deleterious effects of one, three, or even five injections, measured biomechanically (tension to failure) or histologically (light microscopy), compared to controls. This finding should reassure physicians that they are not doing harm with properly placed steroid injections. A 30-year literature review identified eight prospective, placebo-controlled studies of steroid injection treatment for sports-related tendinitis.12 Three of the studies showed beneficial effects of injections at clinical follow-up. A meta-analysis of properly designed investigations of steroid injection for Achilles tendinitis found no beneficial effects,13 although very few studies qualified as rigorous. Adverse side effects occurred with a 1% incidence. No “proof” of the usefulness or uselessness of this treatment modality exists.
Contraindications, Complications, and Side Effects
The lack of a specific diagnosis is the single largest contraindication to a local corticosteroid injection. If the diagnosis is clear and the antiinflammatory effect of a corticosteroid may facilitate the rehabilitation process, injection can be considered.10
Repeated injections to the same area must be avoided, particularly into joints. Alterations in articular cartilage have been documented with repeated administration,14 possibly resulting in joint damage and weakened ligaments.15 A widely recognized complication of steroid injection is tendon rupture, a negative outcome that appears to be decreasing in frequency because it is now well understood. Achilles and other tendon ruptures have been reported,16–26 and deposition of injected material directly into any tendon substance is contraindicated. One report links the effect of repeated steroid injections to rupture of the plantar fascia.27
Some experimental findings have suggested that corticosteroid administration led to smaller, weaker tendons as a side effect.28 A more common side effect is subcutaneous atrophy, especially at the knee and lateral elbow and more frequently with the use of triamcinolone.10 Theoretically, atrophy of the specialized fat pads of the heel following steroid injection for plantar fasciitis may lead to a significant disability in an athlete, due to the loss of cushioning effect.
Alternatives to Corticosteroids
Percutaneous tenotomies have been described for treatment of chronic lateral epicondylitis and plantar fasciitis.18,29 These injections are performed with large bore needles (18 or 20 gauge) under ultrasound guidance. The needle tip is used to repeatedly fenestrate the affected tissue under local anesthetic. The bony surface (i.e., epicondyle) can be abraded and calcifications may be fragmented. This technique is thought to be a safe and effective alternative to corticosteroid injections.18,29
Platelet rich plasma injections use concentrated platelets from autologous blood to stimulate a healing response in damaged tissue. Blood is drawn from the patient and placed in a centrifuge. The concentrated platelets are removed and reinjected directly into the patient’s abnormal musculotendinous tissue or ligament usually under ultrasound guidance. These concentrated platelets produce growth factors that include platelet derived growth factor (PDGF), vascular endothelial growth factor (VEGF), and transforming growth factor-beta (TGF-β). These compounds are instrumental in attracting cells that promote healing by stimulating neovascularization and cellular reproduction.4,5,7,30 The efficacy of PRP injections and appropriate clinical indications (when and where it should be used) are currently being researched and yet to be definitively determined. Initial results of clinical studies appear promising.13,31,32
Methods of Injection
Tendon and tendon sheath injections are office procedures, typically performed under clean or sterile conditions. The corticosteroid of choice is often combined with a local anesthetic, the latter helping to confirm the proper location of the deposited material. Diagnostic ultrasound has been advocated to guide injections near the heel when guidance by palpation alone fails.33





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


