Figure 25.1
Excision of the circular skin disk while applying pressure beneath the abdominal wall protects the underlying bowel
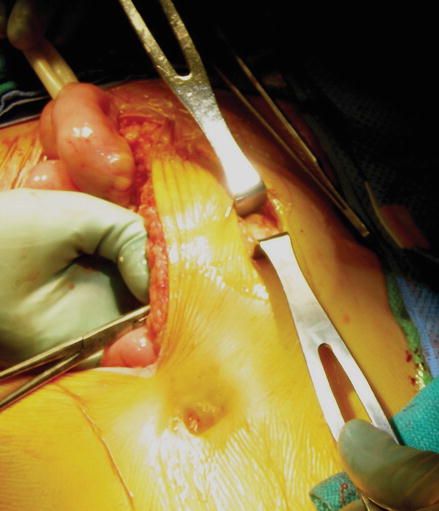
Figure 25.2
Exposure of the anterior rectus sheath using blunt dissection
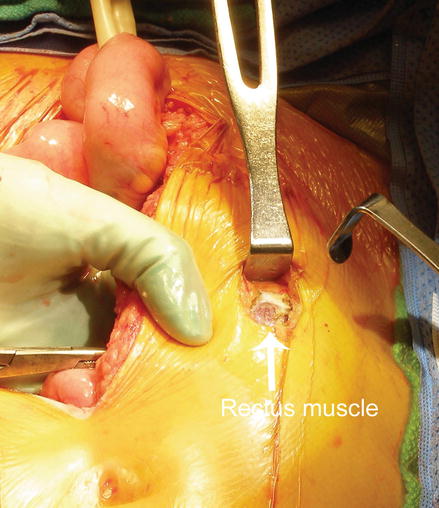
Figure 25.3
Division of the anterior rectus sheath exposing the rectus muscle. The muscle fibers are separated bluntly, but are not divided
Electrocautery is then used to divide the posterior fascia and peritoneum, taking care to protect the underlying viscera. The defect in the fascia should admit two fingerbreadths to allow adequate space for the bowel without vascular compromise. Large fascial defects should be avoided as they are associated with a high rate of parastomal hernia formation [7, 8].
The bowel segment is gently retrieved from the peritoneal cavity with a Babcock clamp placed through the hole in the skin, while taking care to avoid pulling the intestine or tearing the mesentery. For loop stomas, gentle traction can be applied by passing a penrose drain adjacent to the bowel wall (Fig. 25.4). The bowel should protrude 2–4 cm from the skin. The abdominal incision is then closed to avoid contamination when the bowel is reopened for stoma maturation.
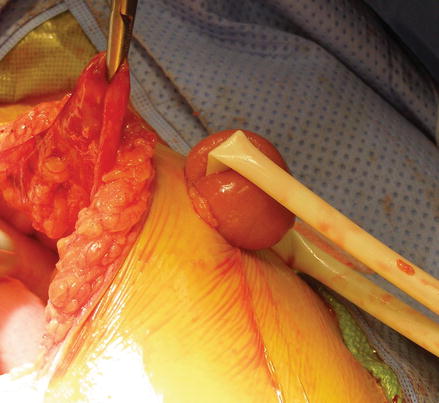
Figure 25.4
Gentle retraction of the bowel through the fascial defect with a penrose drain
First described by Brooke, the stoma is matured by everting the bowel edges [9]. This step allows for the ostomy to easily empty into the appliance away from the skin, protecting the skin and preventing leakage around the appliance. This is especially important for high volume stomas, such as ileostomies. This also prevents stricture formation of the distal bowel. The bowel is then opened by excision the previous staple line in the setting of an end ostomy or opening the bowel on the antimesenteric border for a loop ostomy.
In the case of an end ostomy, 3–4 seromuscular absorbable sutures are placed circumferentially around the bowel lumen to evert the edges. Each suture is passed from inside to outside through the lumen of the bowel including the mucosa and serosa. The next bite is seromuscular at the bowel wall where the abdominal skin and protruding bowel meet. The final bite is through the dermis and each suture is tagged with a hemostat. To evert the edge, the blunt end of a forceps is placed along the bowel wall, and tucked under the stitch. The suture is gently pulled tight and tied as the bowel everts over the forceps and slightly intussuscepts (Fig. 25.5). Once the corners are secure, simple interrupted sutures are placed evenly around the lumen, starting inside-out through the entire thickness of the bowel and into the dermis. A clear stoma appliance is then placed over the everted bowel.
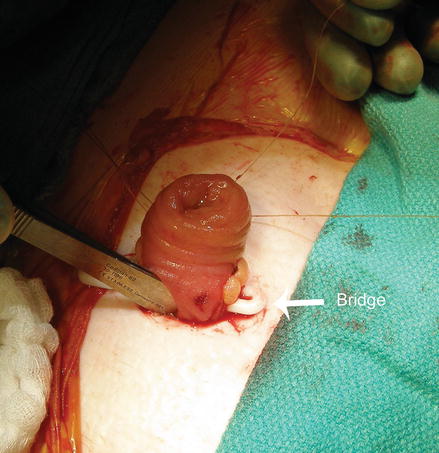
Figure 25.5




Circumferential placement of sutures around the stoma incorporating full thickness bowel wall, serosa, and dermis. Placement of a bridge to temporarily support the loop ostomy is optional (white arrow)
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
