Figure 19.1
Metal clamps are placed across the distal mesentery in opposite directions with their tips pointing inwards. A Metzenbaum scissors is then used to divide the mesentery sharply. Silk or Vicryl ties are used to ligate the mesenteric vessels. This mesenteric division should occur more proximally when resecting small intestine to remove a malignancy
Hand-Sewn Technique
If the patient is hemodynamically stable, the bowel anastomosis can be performed using either a hand-sewn or stapled technique. A hand-sewn anastomosis may be performed in an end-to-end fashion in either one or two layers, as long as the bowel diameters are approximately equal. Alternatively, a side-to-side (functional end-to-end) or end-to-side hand-sewn anastomosis may be performed. There is no difference in leak rate between single and double layer anastomoses [6, 7]; this can be left to surgeon preference. A single layer anastomosis or the inner layer of a two layer anastomosis can be performed with either a running transmural technique or using interrupted sutures. We prefer to use monofilament absorbable suture, often 2-0 or 3-0 polydioxanone (PDS®) suture (Ethicon, Cincinnati OH). It is critical to take full thickness bites to prevent anastomotic breakdown or leakage as the submucosal layer of the small bowel provides strength to the anastomosis [1]. The outer layer of suture closure is performed in an interrupted Lembert fashion using braided permanent suture, typically 3-0 silk suture.
Stapled Technique
Stapled anastomoses are typically faster than hand-sewn and are associated with equivalent rates of clinically evident leakage, morbidity, and post-operative mortality [8, 9]. The proximal and distal segments of bowel are aligned in a side-to-side fashion and two silk sutures are placed, one at the staple line and the other more distally, to temporarily secure the two segments in proper alignment (Fig. 19.2). Small enterotomies are then made on the anti-mesenteric side of each segment near the resection edges. A linear stapling device (e.g. GIA stapler) of either 60 or 80 mm is then inserted with one arm through each enterotomy (Fig. 19.3). After confirming that the mesenteries of the bowel segments are outside of the stapling device, it is closed and fired creating a large enteroenterostomy. The stapler is removed and an Army Navy retractor can be used to inspect the luminal staple line for hemostasis. If the patient is on therapeutic anticoagulation, a running monofilament absorbable suture can be placed along the luminal staple line to reinforce the area and assure hemostasis (Fig. 19.4). The common channel enterotomy can then be closed using a hand-sewn technique as above or by firing across the enterotomy with a stapler (either a TA or GIA stapler) (Fig. 19.5). Some surgeons choose to oversew the staple lines with interrupted Lembert braided permanent sutures to create a second layer (Fig. 19.6). Most surgeons place one or more braided sutures distally to reinforce the end of the staple line where the two bowel segments diverge. Depending on its size, the mesenteric defect can then be closed using either running or interrupted braided absorbable sutures, taking care not to injure the blood vessels running through the mesentery (Fig. 19.7).
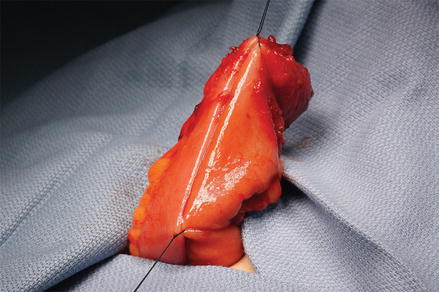
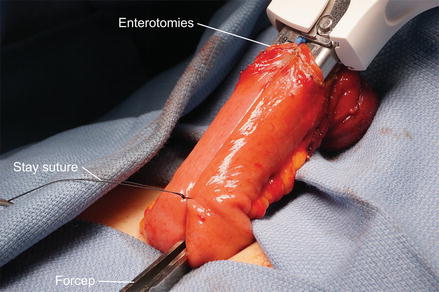
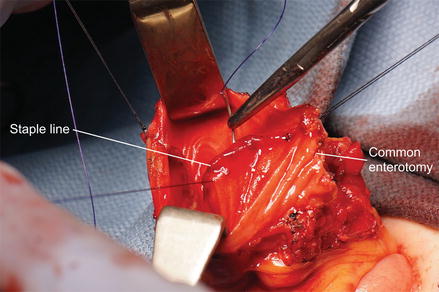
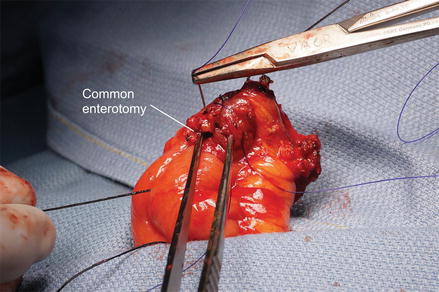
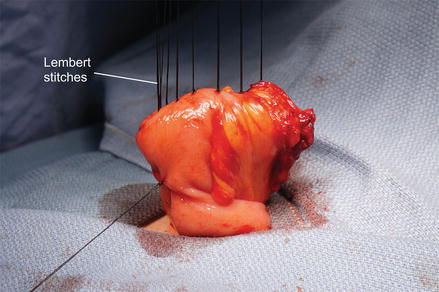

Figure 19.2
Silk stay sutures are placed at the proximal and distal aspects of our side-to-side small bowel anastomosis to assist in maintaining alignment during stapler placement
Figure 19.3
Small enterotomies are made on the antimesenteric side of each small bowel limb. The arms of a GIA stapler are then passed into the enterotomies and the stapler is advanced as shown with the tips pointed downwards. The silk stay suture is used to pull the small bowel upwards toward the handle of the stapler. A debakey forcep is used to retract downward on the mesentery in between the two stapler arms to ensure that the mesentery is not caught within the staple line
Figure 19.4
Army Navy retractors are used to expose the mucosal aspect of the staple line to assess for bleeding. If hemorrhage is noted or the patient is on systemic anticoagulation, the staple line be oversewn with a running PDS suture as shown
Figure 19.5
The common enterotomy is then closed with a Connell stitch using 3-0 PDS. Care must be taken to take full thickness bites with each pass of the needle. The Connell stitch provides hemostasis as well as inverting the bowel wall inwards so that the serosal edges are approximated. The common enterotomy can also be closed with a running stitch or a stapling device
Figure 19.6
Interrupted silk sutures are then placed in the Lembert fashion to create the second layer of a double layer anastomosis. Lembert sutures are often also placed along the staple line laterally and a final silk suture is placed at the most distal aspect of the staple line to reduce tension on that area
Figure 19.7




The completed anastomosis. The size and patency of the anastomosis can be assessed by placing the thumb and forefinger on either side of the completed anastomosis and gently pinching them together
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
