Chapter 38 Skin and Soft Tissue Infections
General Principles
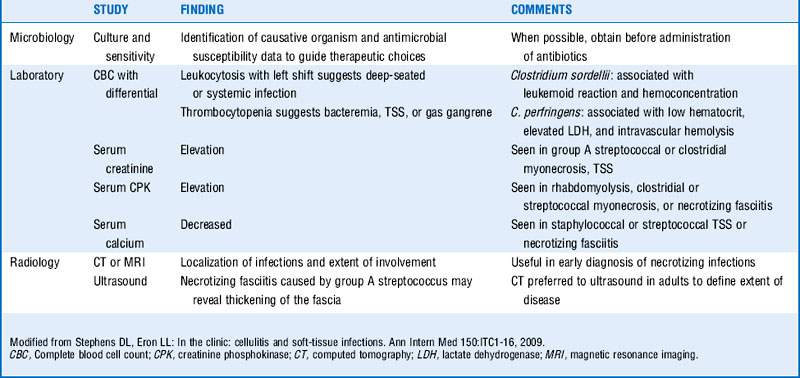
1 If patients with skin or soft tissue infection are seen with signs of systemic toxicity, what laboratory studies should be undertaken?
Blood cultures, cultures of drainage from skin infection site, complete blood cell count with differential, and serum creatinine, bicarbonate, creatine phosphokinase, glucose, albumin, and calcium levels should be obtained. (See Table 38-1.)






3 Which common causative organisms have shown emerging antibiotic resistance?


Cellulitis


6 Lack of response to initial therapy could signify what?
 If a patient does not respond to initial therapy, consider the possibility of resistant strains, atypical organisms, deeper processes such as necrotizing fasciitis or abscess (which may require surgical intervention), as well as underlying conditions such as diabetes, chronic venous insufficiency, or lymphedema (which may slow the clinical response to antimicrobial therapy).
If a patient does not respond to initial therapy, consider the possibility of resistant strains, atypical organisms, deeper processes such as necrotizing fasciitis or abscess (which may require surgical intervention), as well as underlying conditions such as diabetes, chronic venous insufficiency, or lymphedema (which may slow the clinical response to antimicrobial therapy).

7 What risk factors predispose individuals to development of cellulitis?






8 What organisms are associated with cellulitis in:
 Cat or dog bites? Pasteurella multocida, Capnocytophaga canimorsus
Cat or dog bites? Pasteurella multocida, Capnocytophaga canimorsus
 Fresh water exposure? Aeromonas hydrophila
Fresh water exposure? Aeromonas hydrophila
 Saltwater exposure? Vibrio vulnificus and other vibrios
Saltwater exposure? Vibrio vulnificus and other vibrios
 Exposure to fish farming and aquaculture? Streptococcus iniae
Exposure to fish farming and aquaculture? Streptococcus iniae
 Exposure to meatpacking or shellfish? Erysipelothrix rhusiopathiae
Exposure to meatpacking or shellfish? Erysipelothrix rhusiopathiae
 Preorbital cellulitis in children? Haemophilus influenzae
Preorbital cellulitis in children? Haemophilus influenzae
 Hosts with deficiencies in cell-mediated immunity? Cryptococcus neoformans
Hosts with deficiencies in cell-mediated immunity? Cryptococcus neoformans

Cutaneous abscesses
9 How are abscesses managed?
 Large abscesses should be incised and drained, with careful attention to the potential for loculated cavities (and the disruption of these cavities through probing of the pus pocket).
Large abscesses should be incised and drained, with careful attention to the potential for loculated cavities (and the disruption of these cavities through probing of the pus pocket).
 Once drained, the lesion can be left packed or unpacked depending on its extent.
Once drained, the lesion can be left packed or unpacked depending on its extent.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


