Structure of influenza virus (http://www.cdc.gov/flu/images/influenza-virus-fulltext.jpg accessed 25/2/2013).
Influenza viruses are single stranded RNA viruses that make up three genera (Influenza A, B and C) of the family orthomyxoviridae.
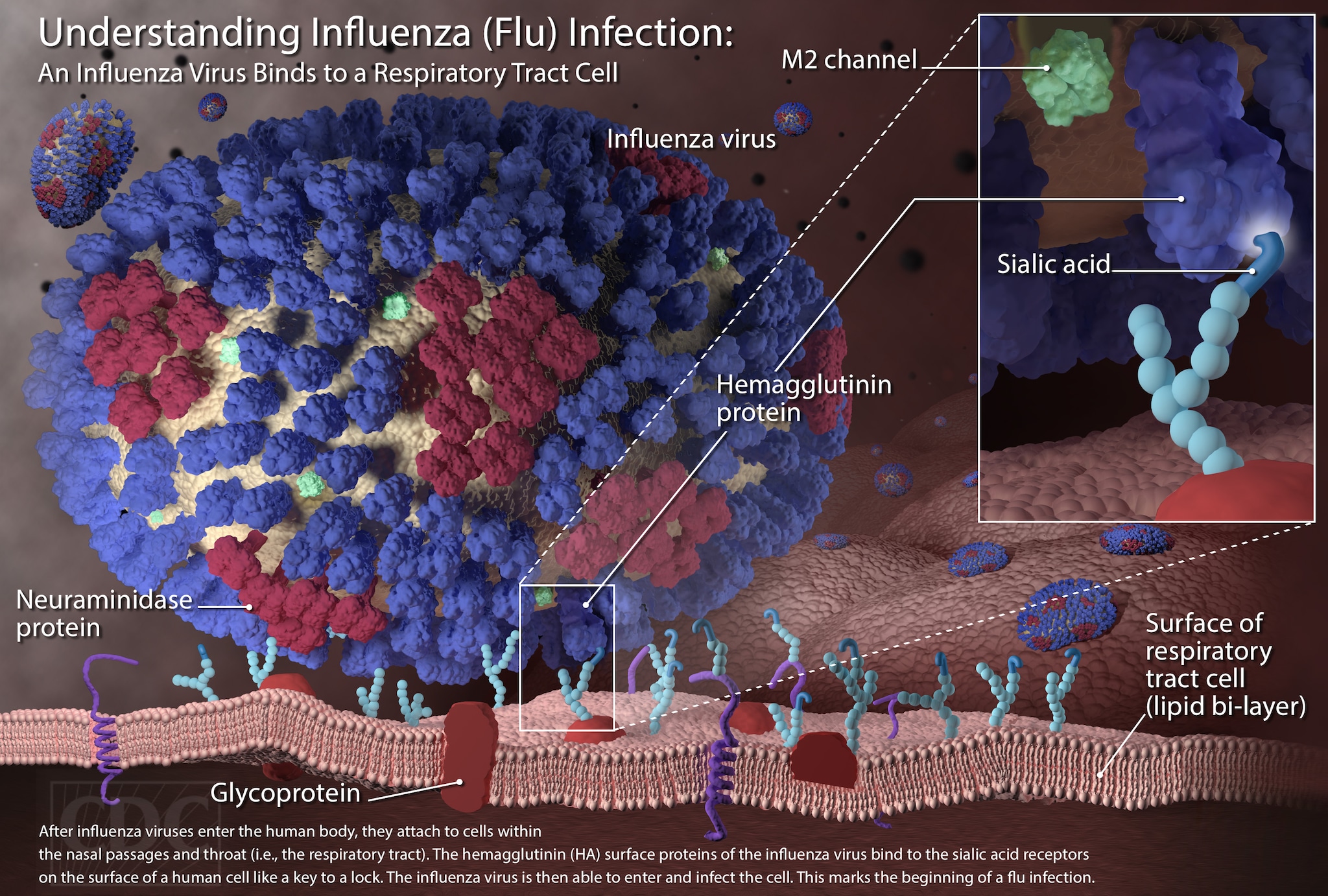
Structurally the influenza virus consists of the following key components:
1 Central core of RNA (eight segments for A) genome and other viral proteins
2 Viral envelope containing two major types of glycoproteins:
Haemagglutinin (HA) enables virus binding to the target cell surface receptor sialic acid, enabling entry of the viral genome into target cells by membrane fusion. Sialic acid-presenting carbohydrates are present on several cell types in the respiratory tract, gastrointestinal tract, heart and brain.
Neuraminidase (NA) acts as an enzyme, cleaving sialic acid from the HA molecule and therefore facilitating release of viral progeny from infected host cells.
Both cell-surface proteins initiate host antibody responses and allow serotyping of virus. NA is also a target for antiviral treatment.
Influenza A
This genus has one species (influenza A virus). Natural hosts include wild aquatic birds, poultry, pigs and humans. Transmission of the virus to other species can result in devastating outbreaks (e.g. poultry and human pandemics). Influenza A is the most virulent human pathogen, causing both epidemics and pandemics. The virus is divided into multiple serotypes based on the antibody response to the surface glycoproteins HA and NA. Human infection is restricted to H1–3, N1–2 serotypes.
Influenza B
This genus has one species (influenza B virus) with one serotype. It affects predominantly humans, but is less common than influenza A and results in milder illness. Its limited host range and limited antigenic diversity means influenza B can cause epidemics, but not pandemics.
Influenza C
This genus has one species (influenza C virus) and results in only occasional human infection.
Transmission
Infection is normally transmitted in three ways:
1 Airborne – aerosols produced by coughing or sneezing
2 Direct transmission of infected mucus with infected nasal secretions
3 Contaminated surfaces and bird droppings – hand-to-eye, hand-to-mouth and hand-to-nose.
Virus shedding when a host individual is infective starts the day prior to symptom onset and continues for approximately 5–7 days.
Antigenic drift and epidemics
During viral replication, no RNA proofreading takes place with point mutations occurring approximately once every newly replicated RNA. This leads to subtle changes in viral surface antigen, helping to evade previously acquired host immunity. This results in seasonal variation in virus. Seasonal flu is normally caused by influenza A and B and peaks in December–March each year in the UK. A new vaccine is required each year.
Antigenic shift and pandemics
Influenza virus RNA is made up of 7–8 segments. If different influenza A viruses infect one cell it can lead to a re-assortment of RNA segments and a whole new sub-type of surface antigen can result. This provides pandemic potential. Pandemics are infrequent, but recurrent worldwide outbreaks of influenza. They are caused by antigenic shift or direct transmission of an avian virus to humans.
There were three twentieth-century influenza pandemics resulting in millions of deaths, e.g. Spanish influenza (1918–20, H1N1 sub-type, 40+ million deaths), Asian influenza (1957–58, H2N2 sub-type, 1+ million deaths), Hong Kong influenza (1968–9, H3N2 sub-type, 1 million deaths).
Influenza A H1N1 2009
This influenza A virus emerged in Mexico in February 2009 and was the result of multiple re-assortment events between swine viruses leading to a novel gene mix not previously reported in swine or human influenza viruses. Pandemic status was declared by the WHO in June 2009 and lasted until August 2011.
The pandemic was considered mild with the majority of infected individuals experiencing a self-limiting illness (50% symptom resolution within 7 days). However > 16,000 individuals died. Pneumonia was present in up to 40% of cases admitted to hospital in the USA with viral pneumonitis or ARDS evident in nearly half of patients admitted to ICU in Australia and New Zealand and secondary bacterial pneumonia present in 20%.
H1N1 remains one of the seasonal influenza viruses in circulation globally.
Influenza in pregnancy
The increased risk of influenza during pregnancy is well recognized. In the 1918 pandemic and in a series of 1350 pregnant women, over 50% developed pneumonia and over half of these died with an overall case fatality of 27%. Half of those women of childbearing age who died were pregnant in the 1957 pandemic.
Pregnant women do not have a higher incidence of seasonal influenza but hospitalization rates are 18-fold that of healthy non-pregnant women of childbearing age.
In the 2009 H1N1 pandemic there was a fivefold higher rate of hospital admission in pregnant women vs. the general population, with the risk of mortality for pregnant women sevenfold that of non-pregnant women of the same age. The WHO reported pregnant women accounted for 7–10% of all hospital admissions with influenza. There were 12 maternal deaths in the UK between April 2009 and January 2010.
Infection is more common in the second and especially third trimesters and risk is further increased in the presence of other risk factors (see later). Pregnant women are more likely to deliver preterm and their babies are more likely to be stillborn or die in the first week of life if admitted to hospital with influenza.
Related posts:
 Non-regional analgesia techniques for labour
Anaesthesia for other obstetric indications: cervical suture, external cephalic version, controlled ARM, manual removal of placenta and perineal repair
Endocrine disease in pregnancy, including diabetes mellitus, thyroid and adrenal disease
HIV and infectious disease in pregnancy, including herpes, syphilis and hepatitis
Non-regional analgesia techniques for labour
Anaesthesia for other obstetric indications: cervical suture, external cephalic version, controlled ARM, manual removal of placenta and perineal repair
Endocrine disease in pregnancy, including diabetes mellitus, thyroid and adrenal disease
HIV and infectious disease in pregnancy, including herpes, syphilis and hepatitis
 Haematologic disease in pregnancy
Haematologic disease in pregnancy
 Clinical governance and patient safety
Clinical governance and patient safety
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



{kind=link}