evident. Histologically, prostate cancers are often heterogeneous. Pathologists commonly assign a Gleason score of 1 to 5 to the mostcommon and next-most-common histologic patterns and add the two scores to obtain a Gleason sum ranging from 2 to 10. Cancers with Gleason sums of 2 to 4 are considered well differentiated, 5 to 7 moderately differentiated, and 8 to 10 poorly differentiated (although cancers with sums of 7 in fact behave in an intermediate fashion between moderate and poorly differentiated cancers). Most cancers discovered by screening are Gleason 6 to 7. In recent years, pathologic grading (but not the cancers themselves) has shifted so that few prostate cancers are now graded less than Gleason 6.
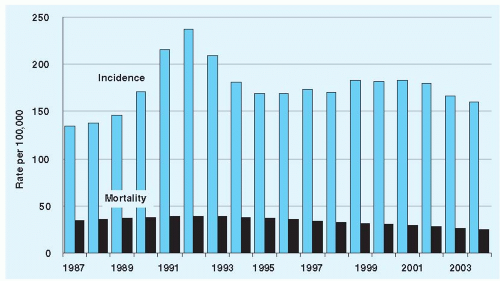 Figure 126-1 Incidence and mortality of prostate cancer in the United States. (From Howlader N, Noone AM, Krapcho M, et al., eds. SEER Cancer Statistics Review, 1975-2008. Bethesda, MD: National Cancer Institute. http://seer.cancer.gov/csr/1975_2008/, based on November 2010 SEER data submission, posted to the SEER web site, 2011.) |
TABLE 126-1 Estimates of 15-Year Outcome Probabilities for Men Diagnosed with Prostate Cancer in the PSA Era, by Age and Gleason Score | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
decrease in overall mortality. The benefit appeared confined to men younger than 65 years old. However, it is important to recognize that men in the Scandinavian trial were generally diagnosed with a nodule or disease that was otherwise clinically evident, with almost half of participants undergoing surgery showing evidence of extracapsular cancer. The recently published Prostate cancer Intervention Versus Observation Trial (PIVOT) randomized 731 men with prostate cancer largely discovered through PSA screening to radical prostatectomy versus observation. After a median follow-up of 10 years, overall and prostate cancer specific mortality were not significantly lower with surgery. However, for the minority of men with more aggressive cancers, such as with a baseline PSA level >10 ng/mL, surgery significantly reduced overall mortality. An ongoing trial in the United Kingdom has a treatment trial (surgery vs. radiotherapy vs. active monitoring) nested within a screening trial.
Related posts:
 Screening for HIV Infection
Screening for HIV Infection
 Screening for Hyperlipidemia and Associated Coronary Heart Disease Risk Factors
Evaluation of Arterial Insufficiency of the Lower Extremities
Evaluation and Prevention of Occupational and Environmental Lung Disease
Management of Chronic Obstructive Pulmonary Disease
Screening for Hyperlipidemia and Associated Coronary Heart Disease Risk Factors
Evaluation of Arterial Insufficiency of the Lower Extremities
Evaluation and Prevention of Occupational and Environmental Lung Disease
Management of Chronic Obstructive Pulmonary Disease
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


