CHAPTER 177
Scabies
(Human Itch Mite)
Presentation
Patients may rush to the emergency department or call for medical help shortly after having gone to bed, unable to sleep because of intense itching. (Severe pruritus, which is the hallmark of this disease, is intensified at night for no known reason.) These patients have skin lesions that include mite burrows, which appear as short (about 2 to 3 mm in length), elevated, gray, threadlike, serpiginous tracks. A small papule or vesicle may appear at the end of the burrow or may occur independently (Figure 177-1). These papules and burrows are chiefly found in the interdigital web spaces (Figure 177-2), as well as on the volar aspects of the wrists, axillae, olecranon area, nipples, waistline, genitalia, and gluteal cleft (Figure 177-3). Nipple pruritus in females is a useful historical clue. Pruritic erythematous papules on the glans penis are characteristics of scabies infestation in males (Figure 177-4). The head and neck are usually spared, but scabies lesions can occur anywhere on the body (Figure 177-5), including the face and scalp. Infants and young children may also have palm and sole involvement with vesicular and pustular lesions. Secondary bacterial infection is often present. Scabies in the elderly may be difficult to diagnose because the cutaneous lesions are often very subtle.

Figure 177-1 Scabies burrow on the side of the foot. (From White G, Cox N: Diseases of the skin, ed 2. St Louis, 2006, Mosby.)

Figure 177-2 Lesions are commonly found in the interdigital web spaces and the sides of the fingers. (From White G, Cox N: Diseases of the skin, ed 2. St Louis, 2006, Mosby.)
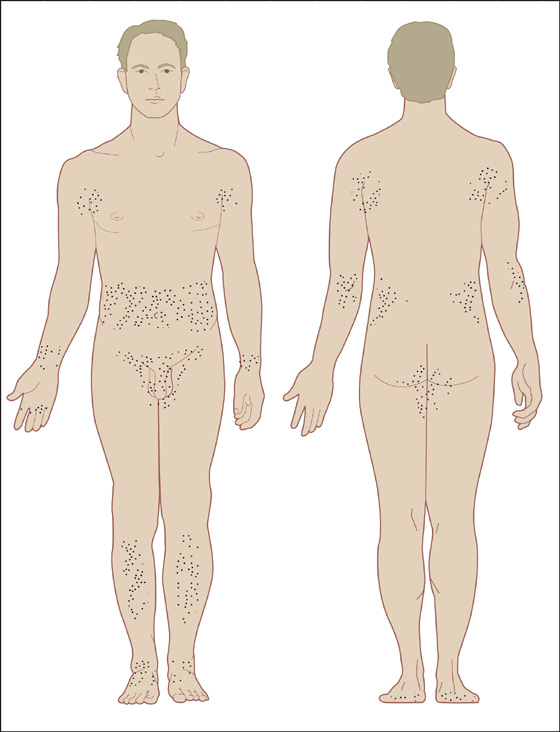
Figure 177-3 Characteristics of distribution of scabies lesions. (Adapted from Goldstein BG, Goldstein AO: Practical dermatology, ed 2. St Louis, 1997, Mosby.)

Figure 177-4 Scabies of the penis causes intense itching and red papules on the glans, which is nearly diagnostic of the disease. (From White G, Cox N: Diseases of the skin, ed 2. St Louis, 2006, Mosby.)

Figure 177-5 Lesions about the umbilicus. (From White G, Cox N: Diseases of the skin, ed 2. St Louis, 2006, Mosby.)
What To Do:
 Attempt to confirm the diagnosis of scabies by placing mineral oil over five or six nonexcoriated suspicious papules or burrows, and scrape or shave them with a No. 15 scalpel blade onto a microscope slide. Examine under low magnification for the mite, its oval eggs, or fecal concretions (scybala). Any one of these findings clinches the diagnosis (Figure 177-6). Burrows can be made more visible by first liberally covering the area with liquid ink and then removing excess ink with an alcohol swab, leaving the burrows stained. If the clinical picture alone is convincing, especially if there is someone else at home (a source) who is itching, treatment should be instituted without the help of microscopic examination, or even in the face of negative scrapings.
Attempt to confirm the diagnosis of scabies by placing mineral oil over five or six nonexcoriated suspicious papules or burrows, and scrape or shave them with a No. 15 scalpel blade onto a microscope slide. Examine under low magnification for the mite, its oval eggs, or fecal concretions (scybala). Any one of these findings clinches the diagnosis (Figure 177-6). Burrows can be made more visible by first liberally covering the area with liquid ink and then removing excess ink with an alcohol swab, leaving the burrows stained. If the clinical picture alone is convincing, especially if there is someone else at home (a source) who is itching, treatment should be instituted without the help of microscopic examination, or even in the face of negative scrapings.

Figure 177-6 Microscopic examination of burrow scrapings showing two oval eggs and multiple brown feces (scybala). (From White G, Cox N: Diseases of the skin, ed 2. St Louis, 2006, Mosby.)
 Prescribe prescription-strength permethrin (Elimite) 5% insecticidal cream, 60 g, for the patient to massage from his head to the soles of his feet at bedtime, and have him leave it on for 8 to 14 hours before washing it off the next morning. Mites tend to persist in subungual areas. The patient should trim fingernails, scrub beneath them, and then apply the scabicide under the nails. Patients should apply a second treatment 1 week later.
Prescribe prescription-strength permethrin (Elimite) 5% insecticidal cream, 60 g, for the patient to massage from his head to the soles of his feet at bedtime, and have him leave it on for 8 to 14 hours before washing it off the next morning. Mites tend to persist in subungual areas. The patient should trim fingernails, scrub beneath them, and then apply the scabicide under the nails. Patients should apply a second treatment 1 week later.
 Oral ivermectin (Stromectol), 0.2 mg/kg as a single oral dose repeated within an interval of 2 weeks, is as effective as a single application of 5% topical permethrin cream. It should be taken on an empty stomach with water. A total of two or more doses at least 7 days apart may be necessary to eliminate a scabies infestation. Ivermectin is currently available in the form of a 3-mg tablet. The safety of ivermectin in children weighing less than 15 kg and in pregnant women has not been established. (Although permethrin is still perhaps the treatment of choice for scabies, this may not be so in future practice. The high cost and extensive surface area of application that is necessary lead to poor compliance, especially in elderly patients. Because of this, ivermectin may soon be considered the drug of choice. Currently, it is still not approved by the U.S. Food and Drug Administration [FDA] for treating scabies.)
Oral ivermectin (Stromectol), 0.2 mg/kg as a single oral dose repeated within an interval of 2 weeks, is as effective as a single application of 5% topical permethrin cream. It should be taken on an empty stomach with water. A total of two or more doses at least 7 days apart may be necessary to eliminate a scabies infestation. Ivermectin is currently available in the form of a 3-mg tablet. The safety of ivermectin in children weighing less than 15 kg and in pregnant women has not been established. (Although permethrin is still perhaps the treatment of choice for scabies, this may not be so in future practice. The high cost and extensive surface area of application that is necessary lead to poor compliance, especially in elderly patients. Because of this, ivermectin may soon be considered the drug of choice. Currently, it is still not approved by the U.S. Food and Drug Administration [FDA] for treating scabies.)
 Crotamiton lotion 10% (60, 480 mL) and crotamiton cream 10% (60 g) (Eurax; Crotan) are approved by the FDA for the treatment of scabies in adults; they are considered safe when used as directed. Massage cream/lotion into entire body from chin down, repeat 24 hours later and then bathe 48 hours later. Crotamiton is not FDA-approved for use in children. Frequent treatment failure has been reported with crotamiton.
Crotamiton lotion 10% (60, 480 mL) and crotamiton cream 10% (60 g) (Eurax; Crotan) are approved by the FDA for the treatment of scabies in adults; they are considered safe when used as directed. Massage cream/lotion into entire body from chin down, repeat 24 hours later and then bathe 48 hours later. Crotamiton is not FDA-approved for use in children. Frequent treatment failure has been reported with crotamiton.
 Sulfur is the oldest known treatment of scabies, and it is the drug of choice for infants younger than 2 months of age and for pregnant or lactating women. It is available as 5% and 10% precipitated sulfur in petrolatum. The cream is applied nightly for three consecutive nights and washed off 24 hours later. The major drawback to sulfur treatment is the unpleasant odor; also, the treatment will often stain clothes.
Sulfur is the oldest known treatment of scabies, and it is the drug of choice for infants younger than 2 months of age and for pregnant or lactating women. It is available as 5% and 10% precipitated sulfur in petrolatum. The cream is applied nightly for three consecutive nights and washed off 24 hours later. The major drawback to sulfur treatment is the unpleasant odor; also, the treatment will often stain clothes.
 Secondary infection from scratching, such as impetiginized excoriations, can be treated with mupirocin (Bactroban) cream 2%. Folliculitis, abscess formation, lymphangitis, and cellulitis should be treated with appropriate drainage and antibiotics (see Chapter 163, Chapters 166 and 172).
Secondary infection from scratching, such as impetiginized excoriations, can be treated with mupirocin (Bactroban) cream 2%. Folliculitis, abscess formation, lymphangitis, and cellulitis should be treated with appropriate drainage and antibiotics (see Chapter 163, Chapters 166 and 172).
 Tell the patient that the itching will not go away immediately and that this does not mean that the treatment was ineffective. Dead mites and eggs continue to cause an immune response but will eventually be eliminated during normal cutaneous turnover.
Tell the patient that the itching will not go away immediately and that this does not mean that the treatment was ineffective. Dead mites and eggs continue to cause an immune response but will eventually be eliminated during normal cutaneous turnover.
 An antipruritic agent, such as hydroxyzine (Atarax, Vistaril), 25 to 50 mg q6h, can be prescribed for comfort. Adding a short course of oral prednisone may be most effective when pruritus is severe.
An antipruritic agent, such as hydroxyzine (Atarax, Vistaril), 25 to 50 mg q6h, can be prescribed for comfort. Adding a short course of oral prednisone may be most effective when pruritus is severe.
 Clothing, bedding, and towels should be washed with hot water or dry cleaned or placed through the heat cycle of a dryer to prevent reinfection. An alternative method is to place all bedding and clothing that might be infested in sealed plastic bags for at least 72 hours. Thorough cleaning of the patient’s room is recommended.
Clothing, bedding, and towels should be washed with hot water or dry cleaned or placed through the heat cycle of a dryer to prevent reinfection. An alternative method is to place all bedding and clothing that might be infested in sealed plastic bags for at least 72 hours. Thorough cleaning of the patient’s room is recommended.
 Family members, frequent household guests, and close physical and sexual contacts should also be treated simultaneously, whether or not symptoms are present.
Family members, frequent household guests, and close physical and sexual contacts should also be treated simultaneously, whether or not symptoms are present.
 Reexamine patients 1 to 2 weeks after initiating therapy to ensure that there is no recurrence.
Reexamine patients 1 to 2 weeks after initiating therapy to ensure that there is no recurrence.
What Not To Do:
 Do not use lindane (Kwell) on infants, young children, or pregnant women or in widespread “Norwegian” scabies, because enough of this pesticide may be absorbed percutaneously to produce seizures or central nervous system (CNS) toxicity. For this reason, lindane is generally no longer recommended for any patient with scabies.
Do not use lindane (Kwell) on infants, young children, or pregnant women or in widespread “Norwegian” scabies, because enough of this pesticide may be absorbed percutaneously to produce seizures or central nervous system (CNS) toxicity. For this reason, lindane is generally no longer recommended for any patient with scabies.
Discussion
Scabies should be suspected in any patient with pruritus.
Scabies has been a scourge among humans for thousands of years. The condition is caused by the mite Sarcoptes scabiei, var. hominis. The adult is barely visible to the naked eye. The organism is an obligate parasite, requiring an appropriate host for survival. The mites subsist on a diet of dissolved human tissue but do not feed on blood. An adult female mite has a tortoise shape and is only about 0.3 to 0.4 mm in size. The male mite is about half the female size. Although mites cannot fly or jump, they can crawl as fast as 2.5 cm/min on warm skin. After mating on the surface of the skin, the gravid female mite dissolves the stratum corneum with proteolytic secretions and then burrows headfirst into the skin. Eggs are laid at a rate of 2 to 3 per day. Both male and female mites have a lifespan of about 1 month. Young mites develop quickly, leaving the burrows to enter hair follicles and skinfolds in which to hide and feed. They mature within 10 to 14 days, after which mating takes place, beginning a new cycle. Mites can live only up to 3 days off a host’s body environment.
A delayed hypersensitivity reaction to the mites, their eggs, saliva, and scybala (packets of feces) occurs within approximately 2 to 6 weeks of infestations. This inflammatory reaction is responsible for the intense pruritus (the hallmark of this disease). Although scabietic lesions are uncommon above the neck in children and adults, infants may have involvement of the face (Figure 177-7). Scabies in an infant usually means that a close adult contact is the source of the infection.

Figure 177-7 Scabies in an infant involving the face. (From White G, Cox N: Diseases of the skin, ed 2. St Louis, 2006, Mosby.)
Scabies is transmitted principally through close personal contact but may be transmitted through clothing, linens, or towels.
Less than 25% of cases show the characteristic 2- to 3-mm serpiginous tracks. Another method of detecting scabies, other than skin scrapings, is video dermatoscopy. This is noninvasive in vivo visualization of the skin at magnifications of up to 600 × to detect signs of infestation (mites, eggs, and feces).
Families may acquire canine scabies when a puppy is brought into the home. The distribution of lesions on humans infected with dog scabies is distinctively different from that of the human variety. A child who hugs an infested family pet will make greatest contact with his trunk and arms, and most eruptions are thereby seen in this distribution. Canine scabies manifests itself within 24 to 96 hours. It is generally self-limiting in humans, because the mites cannot complete their life cycle and therefore do not survive for more than a few days on a foreign host. For those patients who are unwilling to wait for this form of scabies to resolve on its own, 5% permethrin applied topically is the treatment of choice. The assistance of a veterinarian is recommended for treating the pet.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


