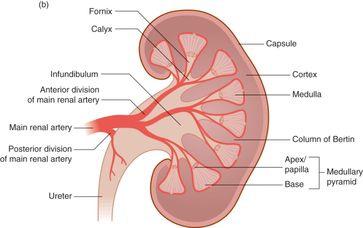
Figure 9.1 Anatomy. (a) The kidneys, ureter, and bladder. (b) The structure of the kidney itself, including the cortex and medulla. Artwork created by Emily Evans © Cambridge University Press.
The ureters course from the renal hilum, descend along the posterior aspect of the lateral pelvic walls, and cross into the pelvic brim at the bifurcation of the iliac arteries. After crossing the pelviureteric junction, they turn anteriorly and medially towards the trigone of the bladder, where they enter. The bladder lies posterior to the pubic bone and anterior to the uterus and rectum in females. It is considered a pelvic organ, but the superior surface, or the dome of the bladder, is intraperitoneal. However, in young children the entire bladder may still be located in the abdomen.
Technique
Point-of-care questions
Transducer selection and orientation
The transducer selection for visualizing the kidney depends on the age of the patient. For the most part, the lower-frequency (2–5 MHz) transducers are utilized; either the curvilinear or phased-array transducers. The phased-array transducer offers a smaller footprint, and is ideal for smaller children. In infants, a higher-frequency, linear transducer may be utilized, offering the greatest resolution without sacrificing the field of view.
For imaging of the kidneys, the transducer is placed at the right upper and left upper quadrants. The kidney lies directly next to the liver on the right side, and next to the spleen on the left side of the body. The indicator is oriented towards the patient’s head, along the midaxillary line. Due to the oblique positioning of the kidneys, it is important to rotate the transducer indicator approximately 10° posteriorly, in order to allow for the adequate visualization along the long-axis of the kidney (Figure 9.2a). Alternatively, for a more direct approach of imaging the kidney, the patient may be rolled on his/her side and the transducer placed on the back (Figure 9.2c). It is important to note that, in relation to the right kidney, the left kidney is located more superior and more posterior. On the patient’s left side, the kidney is often 1–2 cm more superior than on the right side (Figure 9.2b). The transducer may even come close to touching the patient’s bed in order to get the ideal view of the left kidney. After viewing the kidney along its longitudinal axis, the transducer is then rotated 90° in order to obtain the transverse or short-axis view (Figure 9.3a).
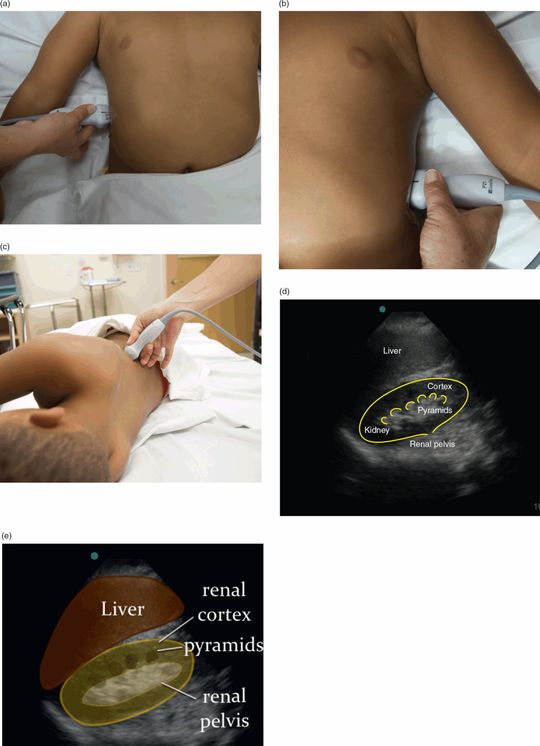
Figure 9.2 Renal imaging, longitudinal view. (a) Right transducer placement, with the indicator oriented towards the patient’s head, at a slightly posterior oblique angle, to be in the plane of the kidney. (b) Left transducer placement. Note that the left kidney is located superior and posterior when compared with the right kidney. (c) Alternatively, the transducer may be placed at the back for a more direct approach to scanning the kidneys. (d) Ultrasound image of the longitudinal kidney. (e) Illustration highlighting important structures visualized on the ultrasound image. Illustration by Laura Berg, MD.

Figure 9.3 Renal imaging, transverse view. (a) Transducer placement, with the indicator oriented 90° from the longitudinal view, with the indicator oriented posteriorly. (b) Ultrasound image of the transverse kidney. (c) Illustration highlighting important structures visualized on the ultrasound image. Illustration by Laura Berg, MD.
Finally, in order to evaluate the bladder, start by identifying the pubic symphysis. The transducer should be positioned in a transverse orientation (with indicator to the patient’s right side) directly caudad to the pubic symphysis and angled slightly towards the patient’s feet (Figure 9.4a). Then, in order to obtain the sagittal bladder view, the indicator should be rotated towards the patient’s head (Figure 9.5a).
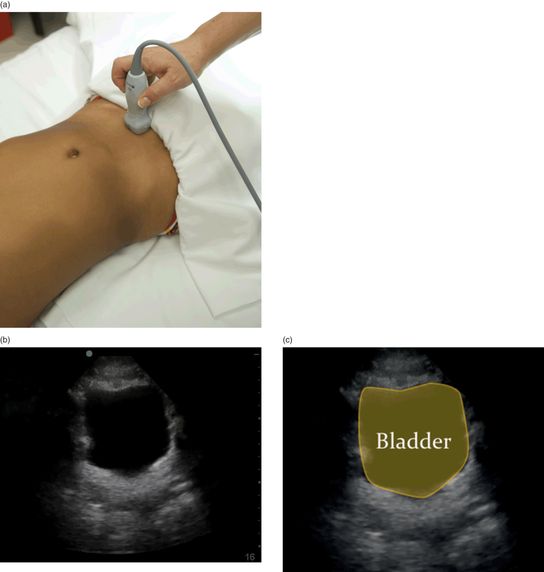
Figure 9.4 Bladder imaging, transverse view. (a) Transducer placement, with the indicator oriented towards the patient’s right side. (b) Ultrasound image of the transverse view of the bladder. (c) Illustration highlighting important structures visualized on the ultrasound image. Illustration by Laura Berg, MD.

Figure 9.5 Bladder imaging, sagittal view. (a) Transducer placement, with the indicator oriented towards the patient’s head. (b) Ultrasound image of the sagittal view of the bladder. (c) Illustration highlighting important structures visualized on the ultrasound image. Illustration by Laura Berg, MD.
Patient position and preparation
Begin the ultrasound examination with the patient in a supine position. Alternatively, patients may be seated upright or in a left lateral decubitus position (Figure 9.2c) in order to displace bowel gas and improve image acquisition. There is no special patient preparation. Proper draping may enhance patient comfort and maintain modesty during the examination of the bladder.
Ultrasound imaging
The renal ultrasound examination consists of both right and left kidneys in two views (longitudinal and transverse), and the bladder in two views (transverse and sagittal). Additionally, color Doppler may be utilized in order to identify ureteral jets in the bladder.
Kidneys
The kidney should be viewed in both the transverse (short-axis) and longitudinal (long-axis) orientations, fanning completely through the kidney in both planes. The sonographic appearance of a normal kidney, in its long-axis, is a kidney-bean-shaped structure, measuring around 5 cm wide and 10 cm long in adults (Figure 9.2c,d). Normal kidneys are usually within 2 cm of each other in size. In the transverse view, the kidney appears in a cross-section, as a “c”-shaped organ surrounding an echo-dense center that represents the collecting system and hilum (Figure 9.3b,c).
The right kidney typically rests in a more inferior position than the left kidney due to displacement by the liver on that side. On the right side of the body, the liver will provide an acoustic window and can serve as a landmark in locating the kidney, which should lie adjacent to and inferior to the liver. On the left side, the spleen provides an acoustic window to view the kidney. It is, however, more challenging to scan the left kidney, since stomach, bowel gas, and rib shadows may interfere with obtaining a clear image. Having the patient take a deep breath and holding it will help displace the kidney inferiorly and out from behind the rib cage in order to create a better image.
The kidney appears hypoechoic, in comparison to the adjacent liver or spleen. Surrounding the kidney is an echogenic capsule called Gerota’s fascia. In between the liver/spleen and Gerota’s fascia is a layer of perinephric fat, which appears hyperechoic, but is less echogenic than Gerota’s fascia. Within the structure of the kidney itself, the renal pyramids in the medulla appear hypoechoic. The calyces appear echodense and converge medially into the echodense renal pelvis. Finally, color Doppler may further elucidate the renal vessels located in the hilum (Figure 9.6).
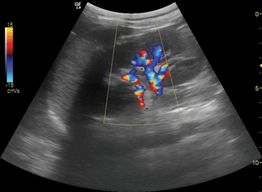
Figure 9.6 Color Doppler of the kidney. Longitudinal view of the kidney, with renal vessels in the hilum illuminated with Doppler color flow.
There are certain sonographic features that are unique to pediatric patients. In the first few months of life, the renal parenchyma may appear isoechoic, or even hyperechoic in comparison to the liver. Outside of the newborn period, a hyperechoic renal parenchyma may be a sign of intrinsic disease or renal failure. In addition, children with healthy kidneys may exhibit prominent pyramids, or a pronounced corticomedullary distinction (Figure 9.7). However, this feature is largely dependent on the quality and resolution of the ultrasound imaging; its absence does not signify renal pathology.

Figure 9.7 Pyramids. Prominent pyramids (P) are especially prevalent in pediatric patients. These may often be mistaken for cysts. The distinguishing feature between pyramids and cysts is that cysts are eccentrically located and often solitary.
Bladder
The bladder should be visualized in both the transverse and sagittal views. In transverse view, the bladder is a centrally located, trapezoidal-shaped, echodense structure surrounded by an echogenic wall (Figure 9.4b,c). In the sagittal view, the bladder appears as a wedge shape (Figure 9.5b,c). Depending on the degree of fullness, the bladder may take on some irregularities in its shape, conforming to the fluid within and pressure from other organs in the pelvis and abdomen.
Ureters
Normal ureters are difficult to visualize throughout their entire course with ultrasound. However, they can easily be visualized as they exit the kidneys. While evaluating the bladder in the transverse orientation, color flow Doppler may be utilized in order to evaluate the ureteral jets for symmetry. Ureteral jets are most commonly located at the inferomedial portion of the bladder (Figure 9.8a,b).
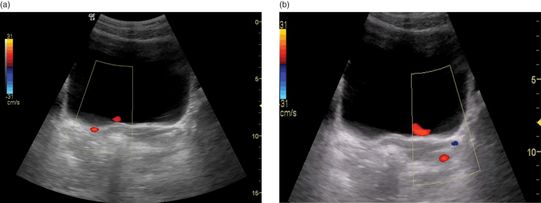
Figure 9.8 Color Doppler: ureteral jets. The ureteral jets are most commonly located at the inferomedial portion of the bladder, and are highlighted in red. (a) Right ureteral jet. (b) Left ureteral jet. Both sides are compared to evaluate for symmetry.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


