(1)
Division of General Internal Medicine, Rutgers Robert Wood Johnson Medical School, New Brunswick, NJ, USA
Abstract
The elderly population is growing rapidly, and the prevalence of anemia is approximately 11 % in the elderly. Observational data demonstrates poor outcome in patients with even mild anemia, but this may reflect the patients’ underlying disease rather than the anemia itself. Clinical trials evaluating transfusion thresholds in the elderly suggest that a restrictive transfusion approach is safe in most clinical settings. Transfusion guidelines do not recommend specific transfusion thresholds in the elderly but rather focus on the hemoglobin level in relation to patients’ comorbidities; thus, transfusion decisions may be affected by the higher prevalence of underlying medical problems in the elderly but not by age itself.
7.1 Introduction
The demographic landscape is changing at a rapid pace. Due to increases in life expectancy, the number of people aged 65 years or older is expected to rise precipitously over the next several decades. According to a 2010 report by the World Health Organization entitled “Global Health and Aging,” the worldwide elderly population is projected to rise from approximately 524 million in 2010 to almost 1.5 billion by 2050. The United States is no exception to this trend; by the year 2030, an estimated 1 in 5 Americans will be elderly, representing about 72 million people. Approximately 89 million Americans will be aged 65 or older by the year 2050, more than doubling the elderly population in 2010.
Anemia is a common condition in the elderly, and thus an important consideration in the medical care of the aging population. According to the NHANES III study, the largest and most comprehensive analysis of the prevalence of anemia in the elderly, 10.6 % of community-dwelling elderly people were found to be anemic (defined as a hemoglobin level <13 g/dL in men and <12 g/dL in women; see Fig. 7.1) [1]. The percentage of anemia in elderly men was slightly higher when compared to that of women (11.0 % vs. 10.2 %).
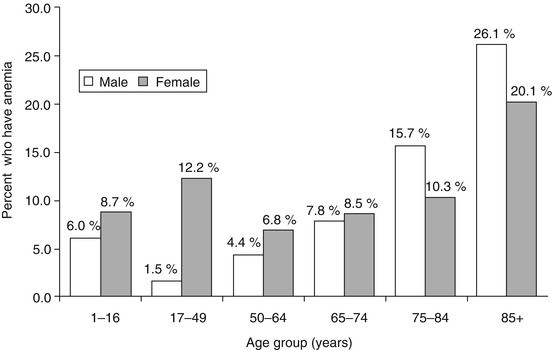
Fig. 7.1
Percentage of people with anemia according to age and sex according to NHANES III
Furthermore, the prevalence of anemia increases steadily with age; in persons older than age 85, about one-quarter of men and one-fifth of women were anemic. These findings are similar to those of other large studies of the community-dwelling elderly population [2–4]. NHANES III also found significant differences in anemia rates in the elderly based on race and ethnicity. Non-Hispanic whites constitute the lowest prevalence (9.0 %), while non-Hispanic blacks constitute the highest (27.8 %).
Clinical data involving institutionalized elderly persons is less robust but indicates a much higher prevalence of anemia. Robinson and colleagues analyzed the charts of 6,200 nursing home residents with a mean age of 83 years old and found a 60 % prevalence of anemia [5]. Additionally, Artz et al. performed a retrospective chart review of 900 skilled nursing facility residents with a median age of 82 years old and found a mean hemoglobin of 12.9 g/dL for men and 11.9 for women [6]. The overall 6-month point prevalence of anemia was 48 %. The discrepancy in prevalence between these two studies is likely due to variations in the patient population studied, but clearly anemia is very common in the institutionalized elderly.
7.2 Etiology of Anemia in the Elderly
The causes of anemia in the elderly are generally divided into the following four categories: (1) nutrient deficiency, (2) chronic disease/inflammation, (3) chronic kidney disease, and (4) unexplained cause. NHANES III showed nearly a one-third split in prevalence between nutrient deficiencies (34 %), anemia of chronic disease (32 %), and unexplained anemia in the elderly (34 %). Half of the cases of nutrient deficiencies were due to iron deficiency (17 % of the total anemic population). Folate and vitamin B12 deficiency each accounted for about 6 % of all anemia. Eight percent of the cases of anemia of chronic disease were deemed secondary to chronic kidney disease. The authors theorized that the large proportion of unexplained anemia was related to the study design in that only a limited laboratory evaluation was performed in the study participants. Etiologies such as hypothyroidism, multiple myeloma, myelodysplastic syndrome, and thalassemia minor were thought to account for a significant portion of the unexplained cases.
A smaller but more intensive study performed by Price and colleagues enrolled 190 elderly patients with anemia from a hematology clinic [7]. All patients underwent a history, physical, laboratory evaluation (including a complete blood count with red cell indices, iron studies, erythropoietin level, and assessment of renal and thyroid function), and review of blood smears. Any further testing was left to the discretion of the treating physician and recorded for inclusion in the study when available. As examples, a serum protein electrophoresis was performed in 87 % of the patients, and a bone marrow biopsy was performed in 17 % of the patients. See Table 7.1 below for their results.
Table 7.1
Etiology of anemia in 190 elderly anemic patients
Etiology of anemia | Frequency (%) |
|---|---|
Anemia of inflammation | 11 (6) |
Hematologic malignancy | 42 (22) |
Suspicious for MDS | 31 (16) |
MDS | 7 (4) |
Others | 4 (2) |
Iron deficiency | 23 (12) |
Therapy for non-hematologic malignancy | 21 (11) |
Renal insufficiency | 8 (4) |
Unexplained anemia | 67 (35) |
Vitamin B12 deficiency | 1 (<1 %) |
Folate deficiency | 0 (0) |
Others | 11 (6) |
Incomplete data | 7 (4) |
Despite a more thorough hematologic evaluation by Schrier et al., a similar rate of unexplained anemia was found as compared to that of NHANES III. However, the more thorough evaluation allowed for identification of several other key causes of anemia in the elderly, including hematologic malignancy and therapy for non-hematologic malignancy. A striking difference emerged between the prevalence of nutritional deficiencies between the two studies, likely due to a more stringent and accurate definition of nutritional deficiencies by Schrier et al. While the NHANES III study looked merely at blood levels of folate and vitamin B12 to make the diagnosis of deficiency, Schrier et al. went a step further in their definition by also requiring a hematologic response to folate or vitamin B12 supplementation.
7.3 Physiologic Response to Anemia in the Elderly
The human body is capable of several adaptive mechanisms in response to anemia [8]. Perhaps most importantly, the adrenergic system is ramped up in order to increase cardiac output and redirect this cardiac output to vital organs via selective arterial vasoconstriction. The renin-angiotensin-aldosterone axis is also stimulated to retain water and sodium. It is reasonable to consider that both of these hemodynamic alterations are vulnerable to attenuation with age. The incidence of heart failure increases with age, growing from about 20 per 1,000 persons between the ages of 65 and 69 to about 80 per 1,000 by age 85 or older [9]. Accordingly, the elderly may be less likely to adequately compensate to anemia by increasing cardiac output. Similar trends in rates of hypertension and peripheral vascular disease are seen with age [10], potentially making increases in vasomotor tone more difficult. This may result in reduced redirection of blood from skeletal, splanchnic, and superficial vessels to cerebral and coronary vessels that is seen in a normal compensation to anemia. All in all, elderly persons may not be able to achieve the hemodynamic changes necessary to fully compensate for anemia.
Several other age-related phenomena have been proposed as mechanisms of increased rates of anemia in the elderly. These mechanisms may also provide insight into the high rates of unexplained anemia seen in the studies mentioned above. Makipour et al. theorized that the following factors may contribute to anemia in the elderly [11]:
1.
Age-related decline in renal function, resulting in decreased erythropoietin levels.
2.
Age-related decline in androgen levels, which has been shown to correlate with a decrease in hemoglobin. For instance, the InCHIANTI study found an association between low testosterone and anemia in an elderly Italian population without cancer or chronic kidney disease [12].
3.
Increased prevalence of chronic inflammatory conditions in the elderly, such as cancer, arthritis, atherosclerosis, and others.
It is worthy to note that another major compensation for anemia is a shift to the right in the oxyhemoglobin dissociation curve. This is made possible by increased production of 2,3-diphosphoglycerate in red blood cells, which results in increased oxygen delivery to tissues at a given partial pressure of oxygen. After a literature search, no recent studies were found that specifically address the effect of aging on the oxyhemoglobin dissociation curve.
7.4 Consequences of Anemia in the Elderly
A review of the literature of the adverse consequences of anemia in the elderly can be broadly divided by the outcomes that were studied. Functional ability, cognitive function, and mortality are three of the most common outcomes studied in this population and are reviewed below. It is important to note that in studies that found worse outcomes in anemic elderly patients, it remains unknown if the anemia itself or the underlying cause of the anemia and/or associated comorbidities is the culprit. We suspect that the underlying cause and comorbidity are responsible for worse outcomes rather than anemia itself.
A number of studies found an association between anemia in the elderly and poor functional status [15–18]. Penninx et al. studied a cohort of 1,146 anemic elderly patients by assessing various markers of physical performance, including a standing balance test, a timed 8-foot walk, and a timed test of 5 chair rises [17]. After adjustment for patients’ baseline performance scores, age, sex, cigarette smoking, blood pressure, and comorbid conditions, anemia was associated with a statistically significant decline in physical performance when compared to a control group. Additionally, separate studies by Penninx et al. showed decreased handgrip and knee extension strength [18] and a higher risk of falls [19] in the anemic elderly.
In addition to its effect on physical performance, anemia in the elderly has been shown to impact cognitive function as well. The Women’s Health and Aging Study showed an association between mild anemia (hemoglobin 10–12 g/dL) and lower executive function in high-functioning, community-dwelling elderly women [20]. In the “Health and Anemia” study, researchers found that anemic elderly persons performed worse on a host of cognitive testing but, after adjustment for possible cofounders, only selective attention remained statistically significant [21]. Hong and colleagues utilized the Health, Aging, and Body Composition study, a prospective cohort of community-dwelling persons aged 70–79, to study the association between anemia and the risk of dementia [22]. Out of 2,552 study participants with available hemoglobin levels, 393 (15 %) were diagnosed with anemia. After 11 years of follow-up, dementia was diagnosed in 23 % of the anemic patients versus 17 % on non-anemic controls. These results remained statistically significant after adjustment for several variables including comorbid conditions. Two earlier studies found similar results with smaller groups of patients and a shorter follow-up period [23, 24].
The most important question is whether anemia in the elderly affects mortality rates. In a study of 755 persons aged 85 and above, risk of mortality was 1.60 (95 % confidence interval, 1.24–2.06; P < .001) in women with anemia and 2.29 (95 % confidence interval, 1.60–3.26; P < .001) in men with anemia after 5 years of follow-up, a finding that remained similar after adjustment for known diseases at baseline [25]. Higher mortality due to malignant neoplasms and infections was found in the anemic cohort. Of note, there was no difference in mortality found from years 5 to 10 of the study.
Mortality in relation to anemia in the elderly was also analyzed using the Cardiovascular Health Study, a cohort of 5,888 community-dwelling elderly persons [4]. After about 11 years of follow-up, mortality rates for those with and without anemia were 57 and 39 %, respectively (P < 0.001). Similarly, the Populations for Epidemiologic Studies of the Elderly cohort was used to show a relative risk of death of 1.61 (95 % confidence interval, 1.34–1.93) when comparing 451 elderly anemic persons to non-anemic persons after adjustment for demographics and baseline comorbidities. This finding remained statistically significant after excluding all patients with certain chronic medical conditions at the onset of the study [26].
7.5 Randomized Controlled Trials of Blood Transfusion in the Elderly
Few large, randomized controlled trials exist on blood transfusions in the elderly. The FOCUS trial by Carson et al., a study of blood transfusions in the postoperative period, provides insight into this question in that nearly all the patients in the study were elderly [27]. This multicenter randomized clinical trial enrolled 2,016 patients aged 50 years or older who underwent surgical repair of a hip fracture with a postoperative hemoglobin level of less than 10 g/dL. Only patients with cardiovascular disease (i.e., history of ischemic heart disease, congestive heart failure, transient ischemic attack, stroke, or peripheral vascular disease or electrocardiographic evidence of a previous myocardial infarction) or cardiovascular risk factors (i.e., hypertension, diabetes mellitus, tobacco history, or a creatinine level above 2.0 mg/dL) were included in the study.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


