5 Radiation Safety for the Physician
Radiation Concepts
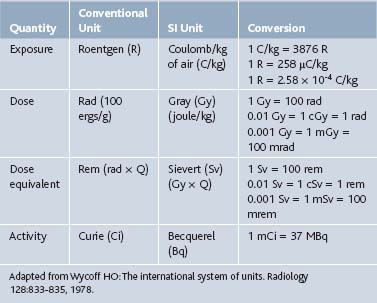
Radiologic nomenclature describes the quantity of radiation in terms of exposure, dose, dose equivalent, and activity. Conventional terms are used in the United States, and an international system of units defined in 1960 by the General Conference of Weights and Measurements is primarily used in Europe. Each system has its unique terms (Table 5-1).1
Terminology
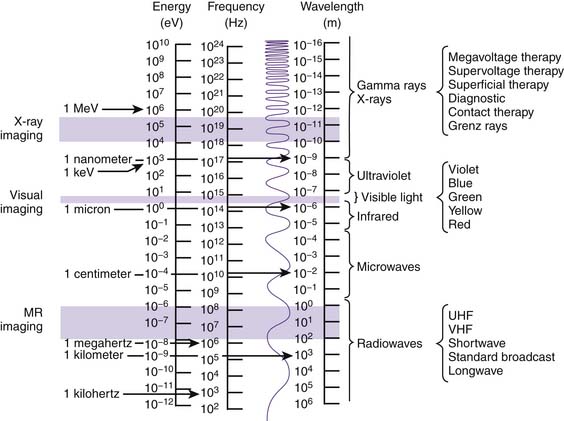
Like matter, energy can be transformed from one form to another. When ice (solid) melts and turns to H2O (liquid) and then evaporates (gas), a transformation of matter has occurred. Similarly, x-rays transform electrical energy (electricity) into electromagnetic energy (x-rays), which then transforms into chemical energy (radiographic image). Electromagnetic energy emitted into and transferred through matter is called radiation. The spectrum of electromagnetic radiation extends more than 25 orders of magnitude and includes not only x-rays, but also the wavelengths responsible for visible light, magnetic resonance imaging (MRI), microwaves, radio, television, and cellular phone transmission (Fig. 5-1).10 Irradiation occurs when matter is exposed to radiation and absorbs all or part of it.
Radiologic Procedures
Fluoroscopy
In general, there are two types of x-ray procedures: radiography and fluoroscopy. Conventional fluoroscopic procedures, such as myelography, barium enemas, upper gastrointestinal series, and swallowing studies, usually are conducted on a fluoroscopic table. The conventional fluoroscope consists of an x-ray tube located above a fixed examining table. The physician is provided with dynamic images that are portrayed on a fluoroscopic screen and the ability to hold and store (“freeze frame”) an image in memory for review or to print as a radiograph (“spot view”) for future reference. Conventional fluoroscopy is considered suboptimal for spinal interventional procedures because of the inability to manipulate the x-ray tube around the patient, and it has been virtually replaced by C-arm fluoroscopes with image intensification for use in spinal injection procedures. The C-arm permits the physician to rotate and angle the x-ray tube around the patient while the patient rests on a radiolucent support table (Fig. 5-2). Image intensification is achieved through the addition of an image-intensifier tube located opposite the x-ray tube. The intensifier receives remnant x-ray beams that have passed through the patient and converts them into light energy, thereby increasing the brightness of the displayed image and making it easier to interpret. In the current image-intensified fluoroscopy, the x-ray tube delivers currents between 1 and 8 mA. Federal regulations limit the maximum output for C-arm fluoroscopes to 10 R/min at 12 inches from the image intensifier.

Factors Affecting Radiation Exposure
Distance
Distance is the most effective means of minimizing exposure to a given source of ionizing radiation. According to the inverse square law, the intensity of the radiation is inversely proportional to the square of the distance. That is, when a given amount of radiation travels twice the distance, the covered area becomes four times as large and the intensity of exposure reduces to 1⁄4 (Fig. 5-3). Therefore, at four times the distance from the source, exposure is reduced to 1⁄16 the intensity.

A rough estimate of the physician’s exposure at a distance of 1 meter from the x-ray tube is 1/1000th of the patient’s exposure.6 It is therefore recommended that the technician and physician remain as far away from the examining table as practical during fluoroscopic procedures. The position of the physician’s body, especially the hands, should be closely monitored and his or her position should be kept at a maximum distance from the fluoroscope at all times.2 For example, it is advisable that the physician deliberately step away from the patient before acquiring each image and also use extension tubing during contrast injection to maximize the physician’s distance from the beam.








