Since its inception in the 1970s, the clinical use of the pulmonary artery catheter (PAC) has been controversial. The PAC provides direct pressure measurements from the right atrium (RA), right ventricle (RV), pulmonary arteries (PAs), and pulmonary capillary wedge pressure as well as a means of measuring cardiac output (CO) by thermodilution. The PAC rapidly gained favor when it was recognized how inaccurate physician assessments of these parameters were. Use of the catheter became widespread, and bedside management was often influenced by the hemodynamic parameters; however, no clinical validation of the benefit of this approach had been performed.
A number of subsequent trials in different patient populations, including surgical patients, patients with acute myocardial infarction, congestive heart failure, and acute lung injury, have shown no benefits, and possibly increased risk, from use of a PAC. A study by the acute respiratory distress syndrome clinical trials network found no differences in outcomes of patients with this syndrome who had their fluid balance guided by use of a central line with central venous pressure monitoring or use of a PAC. Routine use of the PAC should be avoided, but it still has a role in patients with pulmonary arterial hypertension and congenital heart disease, and in patients with complex fluid management issues. In addition, as new therapies emerge, information on treatment benefits may require invasive assessment of hemodynamic parameters.
Newer, noninvasive techniques to assess hemodynamic parameters are being refined and are reducing dependence on the PAC. The clinician using the PAC needs to ask how the information obtained from a PAC will change management of a specific patient, and be alert to possibly the greatest danger of the device: misinterpretation of its hemodynamic measurements. The PAC should be used for the shortest time possible and with the understanding that it is unlikely to alter the clinical course of a patient with multiple complex medical problems (Table 80.1).
PROCEDURE TECHNIQUE
The easiest insertion sites are normally the right internal jugular (RIJ) vein or the left subclavian vein; however, femoral or even brachial vein sites can be used. Prior to starting the procedure, an evaluation of any contraindications to the procedure should be made. In cases with suspected RV dysfunction, pulmonary artery hypertension, tricuspid regurgitation, or RA enlargement, consideration should be given to placing the PAC with fluoroscopic guidance, as direct visualization enhances ability to pass the PAC in difficult cases.
TABLE 80.1 Contraindications to, Indications for, and Complications of Pulmonary Artery Catheter Placement
Relative contraindications
Complications
Left bundle branch block
Complications related to introducer placement:
Severe coagulopathy
Pneumothorax
Hemothorax
Hematoma at site of insertion
Infection at insertion site
Indications (controversial)
Diagnosis and management of shock states
Oliguric acute renal failure Assessment of volume status
Titration of therapy for cardiogenic shock
Diagnosis of PAH
Vasodilator testing in PAH
Diagnosis of multiple cardiac disorders including pericardial constriction, VSD, RV infarction
Perioperative management of major procedures
Complications related to PAC use:
Arrhythmias
Right bundle branch block
Complete heart block (pre-existing left heart block)
The intravenous lines, pressure bags, transducers, and zeroing apparatus should all be assembled and ready prior to the sterile insertion of the PAC. It is useful to have an assistant or nurse available for the procedure. A sterile procedural field should be used, with strict attention to handwashing, mask and cap usage, sterile glove and gown use, as well as full-length drapes. The introducer catheter is inserted in a similar manner to a central venous catheter using the Seldinger technique. The introducer catheter is slightly different in that the dilator is advanced through the introducer rather than as a separate piece of equipment, as occurs with a regular central venous catheter insertion. Additionally, the guidewire and dilator are removed together at the conclusion of the introducer insertion, which leaves the introducer alone in the vessel.
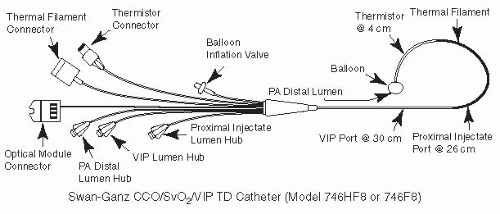
The PAC (Fig. 80.1) should have all ports flushed and the balloon checked for leaks prior to insertion. In addition, the operator should check that the balloon tip does not protrude beyond the inflated balloon as this can increase the risk of vascular rupture. All ports of the PAC should be attached to the pressure transducers and flushed prior to insertion. Waving of the catheter tip prior to insertion with verification of a waveform on the monitor confirms that the catheter ports are correctly attached. Prior to starting the procedure, a final check to verify that the protective catheter sheath has been inserted over the catheter should be performed. The catheter should be oriented prior to insertion to match the natural curve in the catheter to the projected course through the vasculature.
Figure 80.1. Pulmonary artery catheter. (From Clark SL, Phelan JP. Critical Care Obstetrics, 2nd ed. Boston, MA: Blackwell Scientific, 1990:63, with permission.)
The PAC is advanced through the introducer, and when the catheter tip is in the RA, the balloon should be inflated gently. The distance from the insertion site to the RA will vary depending on site, but is usually 15 to 20 cm from the RIJ or left subclavian sites. Once the balloon is inflated and the lock on the inflating syringe has been activated, the catheter is advanced and the waveforms on the monitor are inspected. The RA waveform will increase in amplitude as the RV is entered, which normally occurs at approximately 30 cm (from a RIJ approach). The passage of the catheter through the RV is arrhythmogenic and should not be of prolonged duration. Conversion of the RV waveform to a PA waveform, as the catheter tip traverses the pulmonary valve, is identified by an increase in the diastolic pressure and the development of a dicrotic notch in the tracing (often at 40 cm). Difficulty in traversing the pulmonary valve is not uncommon in patients with pulmonary arterial hypertension from any cause and, if excessive catheter length has been advanced without this transition occurring, the most likely explanation is that the catheter is coiled in the enlarged RV. If this occurs, the balloon should be deflated and the catheter should be withdrawn until an RA tracing is obtained, after which the balloon should be inflated and the procedure attempted again. The pulmonary capillary wedge pressure tracing is identified by loss of the arterial tracing to a flatter tracing of lower amplitude than the PA diastolic pressure (often at 50 cm) (Fig. 80.2 for the pressure tracings obtained as the catheter advances).
Only gold members can continue reading. Log In or Register to continue