CHAPTER 62
Pudendal Nerve Block
Pudendal pain can often be difficult to diagnose and harder to treat. The majority of patients suffering from this malady are female; chronic pelvic pain affects approximately 1 in 7 women.1 Frequently, they have been to various doctors with a complaint of chronic perineal pain that may be localized to the rectum, anus, urethra, or genitalia. This usually causes them multiple diagnoses and treatment without resolution of symptoms. For years, patients with chronic neuropathic perineal pain were assigned a “psychosomatic vulvovaginitis” diagnosis by exasperated physicians.2 Finally, this elusive presentation has been recognized to have a valid biomechanical and a neuropathic basis that allow multiple modalities for its treatment. Current treatments can improve a patient’s quality of life, and research continues to improve outcomes.
DIAGNOSIS
The pudendal nerve is a mixed motor/sensory nerve having numerous potential entrapment sites. Therefore, the clinical presentation varies.
• The pain of pudendal neuralgia (PN) typically waxes and wanes and is often described as burning, tearing, stabbing, sharp, electrical, and shooting along with feelings of a lump or foreign body in the vagina or rectum.3
• Symptoms include abnormal temperature sensations, constipation, pain and straining with bowel movements, straining or burning when urinating, painful intercourse, and sexual dysfunction (including uncomfortable arousal or decreased sensation). PN presents most commonly as unilateral.
• The symptoms are usually aggravated by sitting or cycling and are absent or relieved by standing, recumbent position, and sitting on a toilet seat.4
Indications
Pudendal nerve blocks are used to diagnose and manage patients with chronic pain with possible pudendal origin. Local anesthetic blocks can be used to diagnose pain problems. If the local anesthetic removes the pain, the pain generator is presumed to be distal to this pathology. They can also be used to predict results of surgical neurolysis, pudendal nerve stimulation, and as a direct treatment.
Contraindications
• Systemic infection
• Infections at the skin, injection site, ischiorectal space, rectum, vagina, or perineum
• Coagulopathy
• Contrast allergy (when used)
• Immunocompromised patient
• Metastatic cancer in the area
• Lack of understanding or cooperation with the procedure
Relevant Anatomy
Rising from the sacral plexus and formed from contributions of the second, third, and fourth sacral nerve roots, the pudendal nerve is a sensory and motor nerve. There are 3 branches of the nerve on each side of the body:
• Rectal branch
• Perineal branch
• Penile/clitoral branch
Pudendal neuropathy occurs when the nerve or one of its branches becomes damaged, inflamed, or entrapped.
• The pudendal canal runs from the lesser sciatic notch to the posterior edge of the perineal membrane.
• A space within the obturator fascia, the pudendal (Alcock’s) canal, is bound by the medial aspect of the obturator internus muscle and the lateral wall of the ischioanal fossa.
• It contains the internal pudendal vessels and the pudendal nerves, which enter the gluteal region through the lower part of the greater sciatic foramen.
• The pudendal nerve, when accompanied by the internal pudendal artery, is known as the pudendal bundle. This pudendal bundle courses around the sacrospinous ligament near its attachment to the ischial spine and passes through the ischioanal fossa and then through the pudendal canal.
• Either just before entering the pudendal canal or just within it, the pudendal bundle gives rise to the inferior rectal (inferior anal) nerve, which crosses the ischioanal fossa toward the anal canal and the external anal sphincter muscle.
• Within the pudendal canal, the pudendal nerve divides into two terminal branches, the perineal nerve and the dorsal nerve of the penis or clitoris.3
• Throughout this course, there are two critical areas where compression is likely to occur—at the ischial spine in the gluteal region or in the pudendal canal (Figures 62-1 and 62-2).
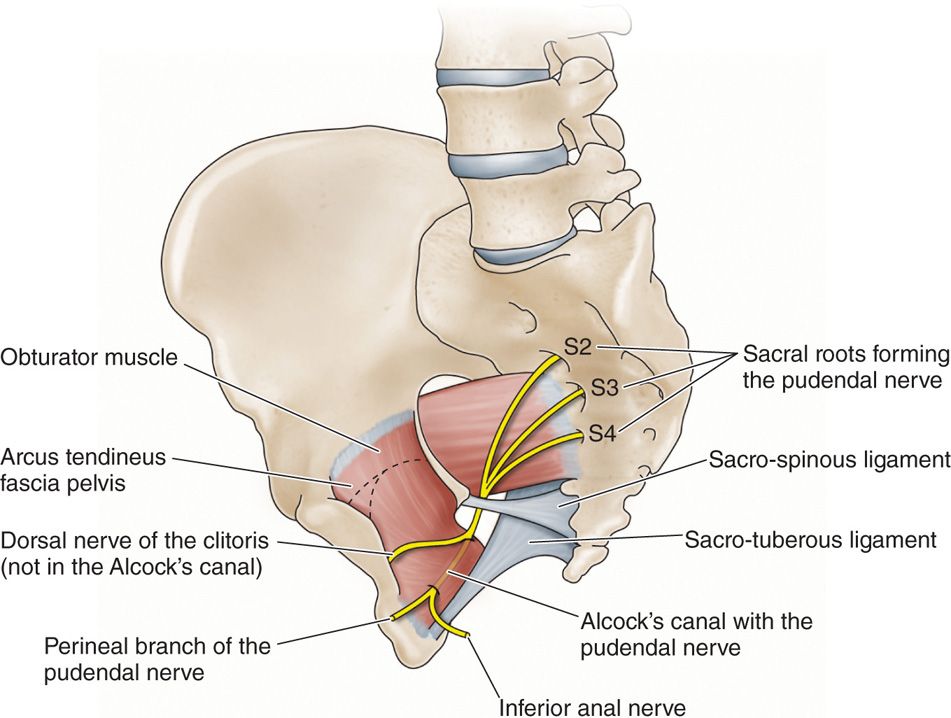
Figure 62-1. The ischial spine3.
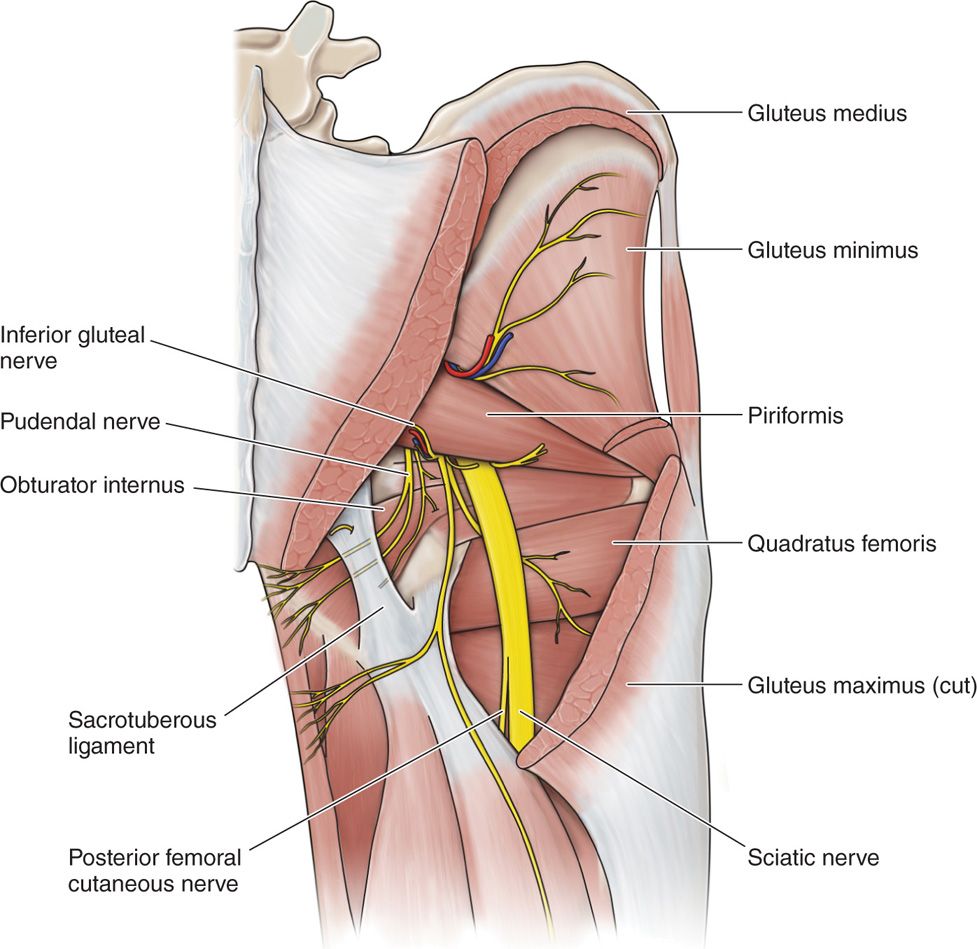
Figure 62-2. Schematic anatomy of deep dissection of gluteal region. Most of gluteus maximus and medius muscles have been removed. Segment of sacrotuberous ligament also has been removed, revealing pudendal nerve. Pudendal nerve emerges from pelvis inferior relative to piriformis muscle and enters gluteal region medial relative to sciatic nerve, superficial relative to sacrospinous ligament, and deep relative to sacrotuberous ligament. After coursing around sacrospinous ligament, pudendal nerve reenters pelvis.10
Diagnostic Criteria5
• Pain in the anatomical distribution of the pudendal nerve
• Pain worsened by sitting
• Patient not woken at night by the pain
• No objective sensory loss
• Positive anesthetic pudendal block
PREOPERATIVE CONSIDERATIONS
Because there are several different approaches, a decision as to the site of damage or entrapment dictates the approach. Injections at the ischial spine anesthetize the entire length of the nerve, but will not address pathology more proximal, at the sciatic notch. The ischial spine can be approached vaginally or transperineally (from a lithotomy position) or from a prone approach, using peripheral nerve stimulation or fluoroscopy or CT guidance or ultrasound. If the entrapment is more distal, injection at the ischium can allow for more selective diagnostic and potentially therapeutic treatment.
Documentation for Off-Label Indications
Not applicable
Fluoroscopic Views
• Supine: AP view of the ischium
• Prone: P view, oblique to the ipsilateral side in order to visualize the ischial spine (Figure 62-3)
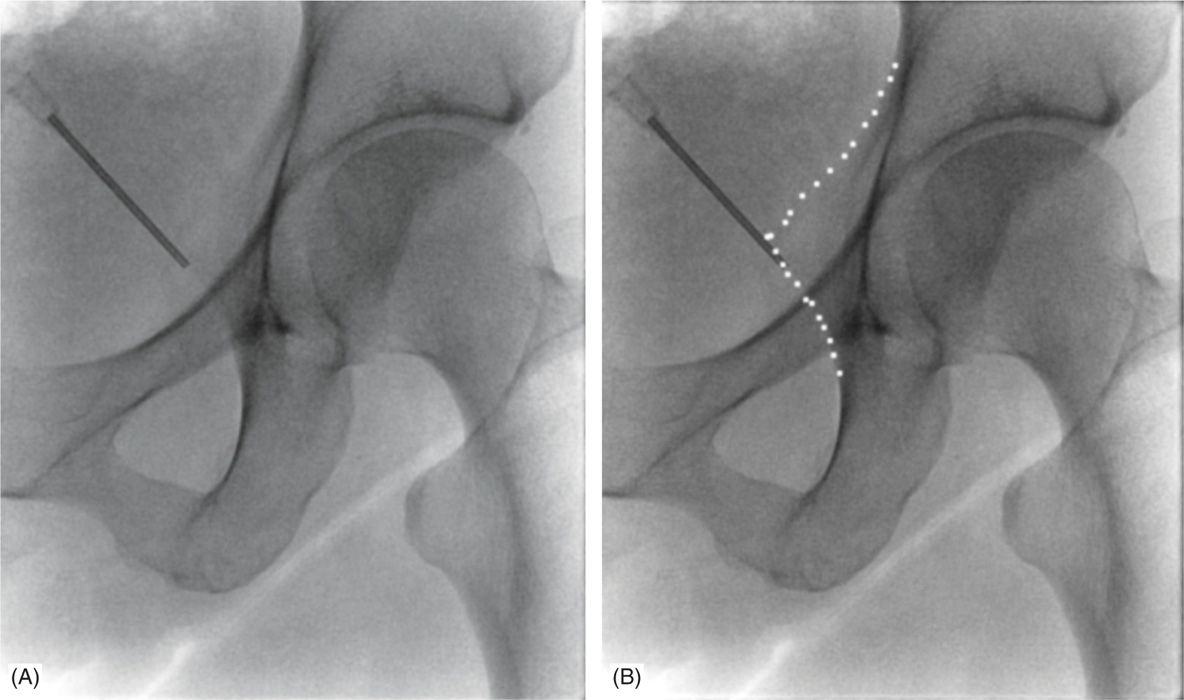
Figure 62-3. Ipsilateral oblique view of the ischial spine. (Used with permission from Andrea Trescot, MD.)
Positioning of Patient
• Depends on approach
![]() Lithotomy for transvaginal or transperineal approach
Lithotomy for transvaginal or transperineal approach
![]() Prone for posterior approach
Prone for posterior approach
Selection of Needles, Medications, and Equipment
• Transvaginal approach
![]() Be sure to use a needle with a guide—either the Iowa trumpet (Figure 62-4) or the Kobak needle guide (Figure 62-5)—to limit the depth of submucosal penetration and to prevent injury to the patient’s vagina and potentially puncturing the physician’s hand.
Be sure to use a needle with a guide—either the Iowa trumpet (Figure 62-4) or the Kobak needle guide (Figure 62-5)—to limit the depth of submucosal penetration and to prevent injury to the patient’s vagina and potentially puncturing the physician’s hand.

Figure 62-4. Iowa trumpet. (Used with permission from Andrea Trescot, MD.)

Figure 62-5. Kobak needle.
![]() Requires a 5-in 22-gauge spinal needle.
Requires a 5-in 22-gauge spinal needle.
• Additional supplies for any approach
![]() 27/30-gauge needle for local infiltration (1% lidocaine)
27/30-gauge needle for local infiltration (1% lidocaine)
![]() 22-gauge 3.5- or 5-in spinal needle
22-gauge 3.5- or 5-in spinal needle
![]() 0.25% or 0.5% bupivacaine, approximately 10 cc (alternatively, 1% lidocaine may be used for quicker onset and shorter duration)
0.25% or 0.5% bupivacaine, approximately 10 cc (alternatively, 1% lidocaine may be used for quicker onset and shorter duration)
![]() Nonionic contrast if dye localization is chosen
Nonionic contrast if dye localization is chosen
![]() Peripheral nerve stimulator (PNS) if chosen to reproduce symptoms
Peripheral nerve stimulator (PNS) if chosen to reproduce symptoms
![]() Fluoroscopy, ultrasound, and/or CT scanner if chosen
Fluoroscopy, ultrasound, and/or CT scanner if chosen
Intraoperative Technical Steps
Transvaginal Approach
• To perform a left-sided block, palpate the ischial spine with the index finger of the left hand, using the Iowa trumpet or Kobak needle guide on the index finger (Figure 62-6).
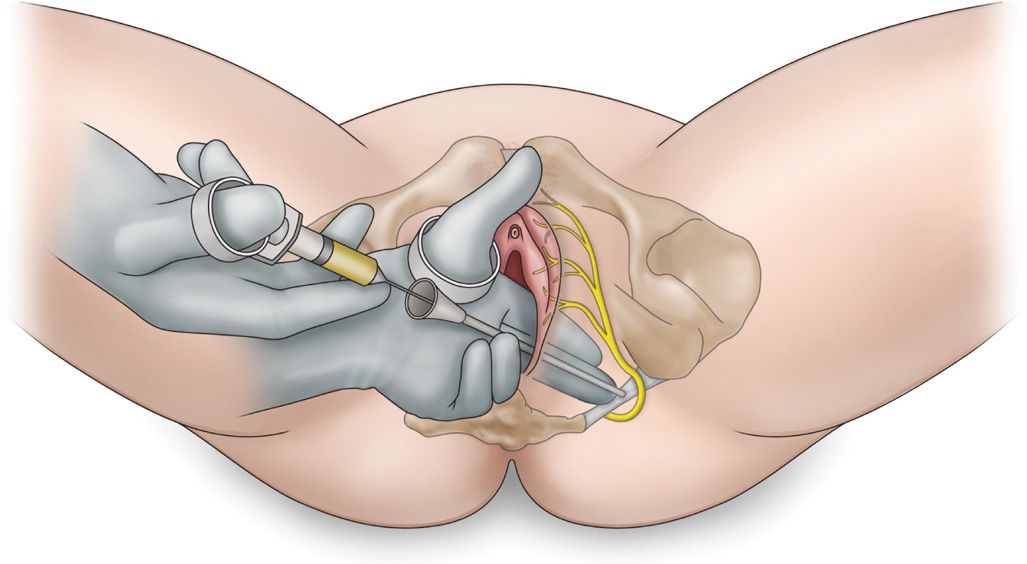
Figure 62-6. Transvaginal approach.6
• Place the end of the guide beneath the tip of the ischial spine.
• Push the needle through the guide into the vaginal mucosa.
• Raise a mucosal wheal with 1 mL of local anesthetic.
• Advance the needle through the vaginal mucosa until it touches the sacrospinous ligament 1 cm medial and posterior to the ischial spine.
• Infiltrate the tissue with 1 mL of local anesthetic.
• Next, advance the needle further through the sacrospinous ligament for a distance of 1 cm until a loss of resistance is appreciated.
• The tip now lies in the area of the pudendal nerve. At this point, the pudendal vessels lie just lateral to the pudendal nerve, so care must be taken to avoid intravascular administration. Aspirate to confirm the needle placement is not intravascular prior to injecting lidocaine.
• Subsequently, withdraw the needle into the guide and move the tip of the guide to just above the ischial spine.
• At this new location, reinsert the needle though the mucosa and again inject.6
• (Note: An alternative to placing the needle through the vagina would be to place the needle lateral to the labia majora but still use the hand transvaginally as a guide.)
Pararectal Approach Using PNS7
• The index finger of the nondominate hand is inserted into the anus and used to palpate the ischial spine, introducing the needle lateral to the rectum down to the ischial spine.
• PNS is used to elicit contraction of the external anal sphincter.
Transperineal Approach Using PNS and Fluoroscopy
• Patient is placed in a lithotomy position, and an AP projection obtained.
• The inferior ramus is palpated through the perineum until a paresthesia is obtained.
• 1 cc of local anesthetic is infiltrated subcutaneously.
• A 22-guage 3.5-in needle is advanced through the perineum under PNS control until the patient identifies a twitch in the distribution of the pain (urethral, vaginal/perineum, rectal) (Figure 62-7).
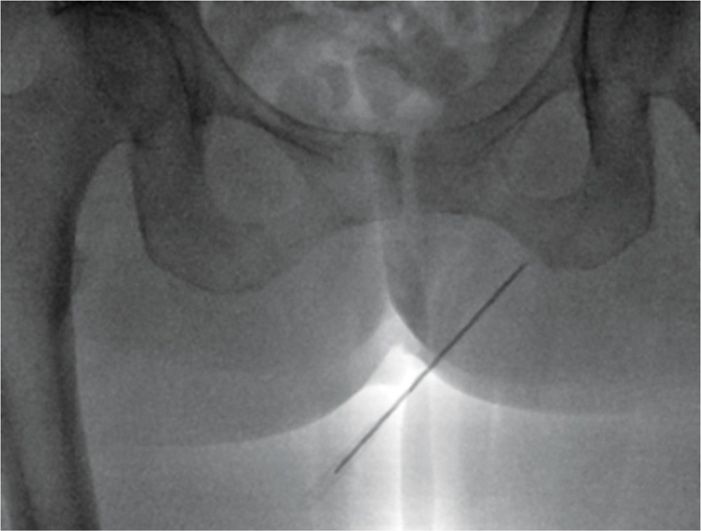
Figure 62-7. Transperineal approach. (Used with permission from Andrea Trescot, MD.)
• Alternatively, for perirectal pain, the patient can be positioned prone in a modified jackknife position.
Posterior Approach Using PNS and Fluoroscopy
• The patient is placed in the prone position.
• The C-arm fluoroscope is projected in the anterior-posterior position and then obliqued to the ipsilateral side to allow visualization of the pelvic inlet and the ischial spine (Figure 62-3).8
• A 22- or 25-gauge 3.5-in needle is then advanced to the tip of the ischial spine and 1 cc of local with deposteroid is injected.
• A peripheral nerve stimulator may help in localization, and contrast confirms the lack of vascular injection (Figures 62-8 and 62-9).
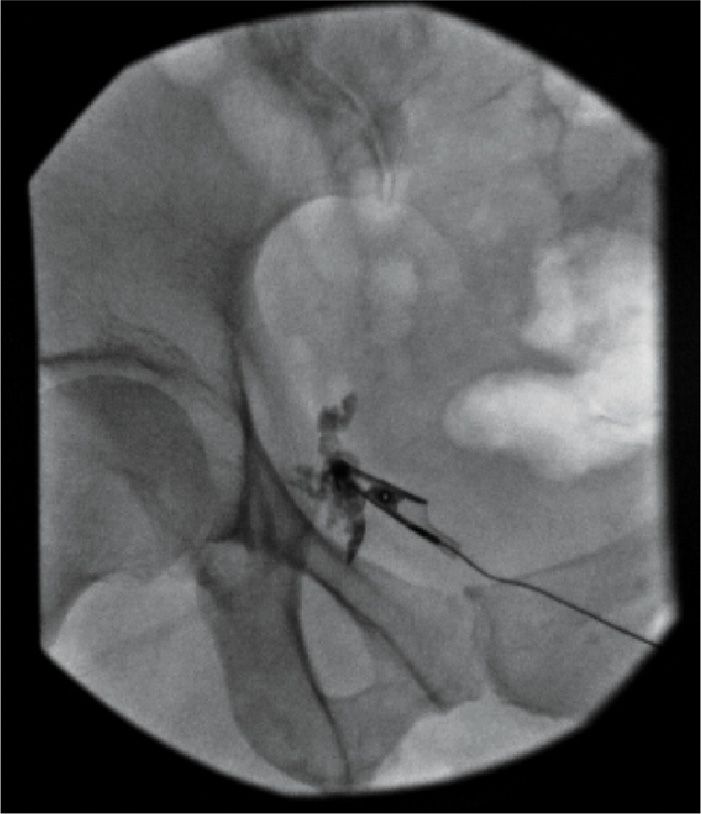
Figure 62-8. Fluoroscopic posterior pudendal injection at the ischial spine. (Used with permission from Andrea Trescot, MD.)
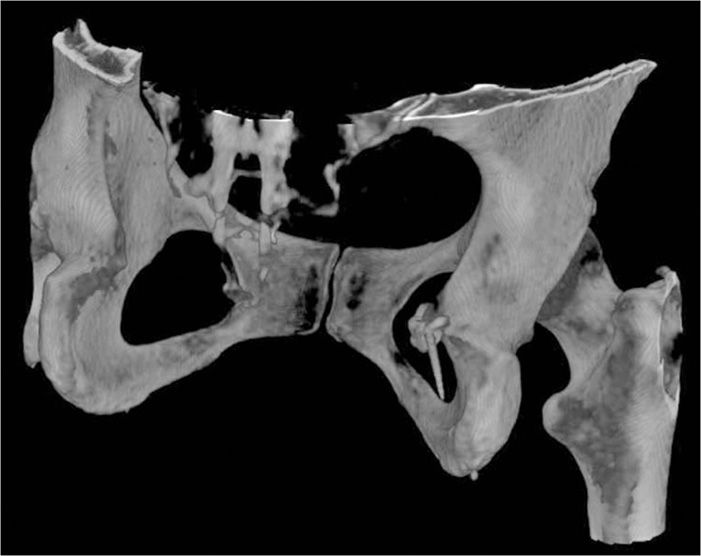
Figure 62-9. 3D reconstruction of fluoroscopic injection. (Used with permission from Andrea Trescot, MD.)
Posterior Approach Using a CT Scan9
• The patient is positioned in the prone position.
• CT images are obtained from the femur head to the ischium.
• Once the ischial spine, sacrospinous and sacrotuberous ligaments as well as the falciform process are located, 1 of 2 approaches may be utilized to block the pudendal nerve.10
• In the first, a 22-gauge needled is placed transgluteally to avoid the sciatic nerve, at the ischial spine between the sacrotuberal and sacrospinal ligament.
• Another approach enters the medial part of the obturator internus muscle under the falciform process.
• After verifying the location of the needle, local anesthetic and deposteroid are then injected (Figure 62-10).
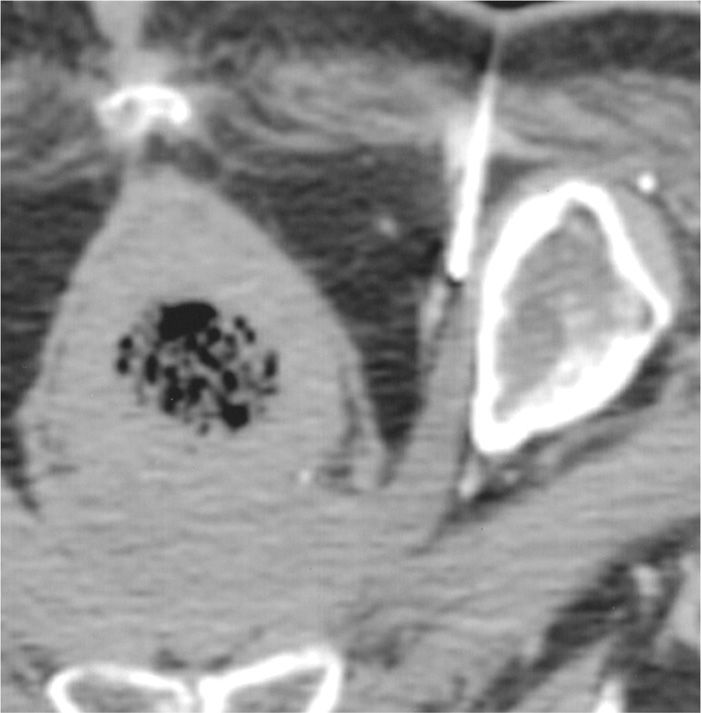
Figure 62-10. CT guided pudendal nerve injection. (Reproduced with permission from American Journal of Roentgenology. Hough DM, Wittenberg KH, Pawlina W, et al. Chronic perineal pain caused by prudendal nerve entrapment: anatomy and CT-guided perineural injection technique. AJR Am J Roentgenol 2003; 181(2):561-7; American Roentgen Ray Society.)
Posterior Approach Using Ultrasound11
• The patient is placed in the prone position.
• A low-frequency curved array US transducer is used in the transverse plane to visualize the ischium forming the lateral border of the sciatic notch.
• By moving the ultrasound probe in a cephalad-caudal direction, the ischium appears as a progressively lengthening hyperechoic line, widest at the ischial spine level.
• The sacrospinous ligament appears as a hyperechoic line in continuity with the ischial spine, with lower echogenicity than bone.
• The sacrotuberous ligament appears as a light hyperechoic line deep to the gluteus maximus muscle, parallel and superior to the sacrospinous ligament.
• Doppler will show the internal pudendal artery close to the ischial spine.
• A 22-gauge spinal or stimulating needle is inserted from the medial aspect of the probe in line to the medial aspect of the artery.
• Once the needle passes through the sacrotuberous ligament (felt as a “click” or “pop”), a small amount of fluid is injected as contrast to confirm location (Figure 62-11).
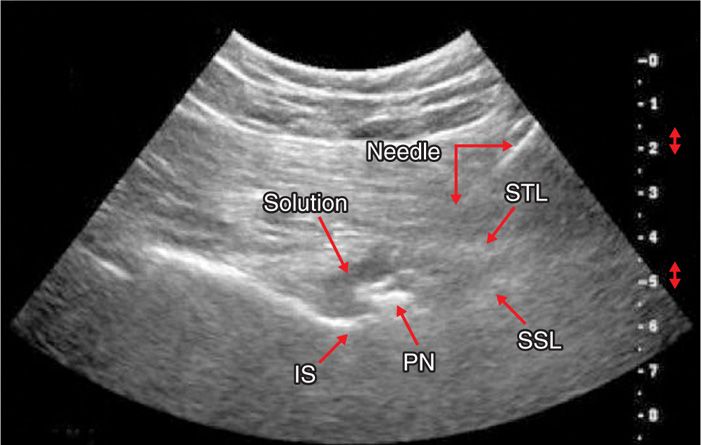
Figure 62-11. Ultrasound pudendal injection. (Reproduced with permission from Rofaeel A, Peng P, Louis I, Chan V. Feasibility of real-time ultrasound for pudendal nerve block in patients with chronic perineal pain. Reg Anesth Pain Med 2008;33:139-45.)
• After verifying the location of the needle, local anesthetic and deposteroid are then injected.
Subsequent Options
• Botulinum toxin. The pudendal nerve has a close relationship with the obturator internus muscle. It has been theorized this relationship could contribute a musculoskeletal component to the pain of pudendal neuralgia. A particular case study from 200512 investigated the effects of botulinum toxin on a patient that had previously been treated with multiple modalities including surgical release. The patient had botulinum toxin injected into the right obturator internus muscle with a 90% relief of symptoms for a period of 3 months. This was a single case study but further investigation is warranted to determine if botulinum is a viable therapeutic option for patients with pudendal neuralgia.
• Cryoanalgesia. In her 2003 review,13 Trescot discusses how cryoanalgesia, cryoneuroablation, or cryoneurolysis is a specialized technique for providing long-term pain relief when pain has been shown to be caused by sensory nerves. The pudendal nerve is approached either vaginally or percutaneously. The vaginal approach is a simple modification of the pudendal nerve block utilized by obstetricians. Using a modified Iowa trumpet with the patient in the lithotomy position, the 2.0 mm probe is advanced through the trumpet to the ischial spine. Cryoneurolysis at this site will lead to profound hypoesthesia, including the possibility of loss of clitoral sensation. The transperineal approach can be much more selective in the isolation of specific branches of the pudendal nerve. If the pain is primarily vaginal, the patient is placed in a modified lithotomy position with the feet on the table instead of in stirrups. The 12-gauge introducer is directed toward the sacrospinous ligament instead of the ischial spine itself, and the 2.0-mm probe sensory stimulation is used to select the stimulation field needed. In the same way, if the pain is primarily rectal, the patient is positioned prone in a jackknife position, placing the 12-gauge introducer and then the 2.0 mm probe more inferiorly, using stimulation to direct the probe toward the rectal branches.
• Radiofrequency. Continuous radiofrequency ablation (CRF) is a percutaneous minimally invasive technique that has been in clinical use for over 25 years. Pulsed radiofrequency ablation (PRF) is a more recent neuromodulatory technique that is felt to be less destructive than conventional CRF. Although the exact mechanism of action for PRF is unknown, current literature supports involvement of electromagnetic fields resulting in neuromodulation. A recent case report14 suggests that PRF may be useful in treatment of refractory pudendal neuralgia.
• Peripheral stimulation. There have been multiple approaches proposed for electrical stimulation to treat chronic pelvic pain—retrograde,15 antegrade through the sacral hiatus,16 transsacral,17 and on the nerve itself.18 Discussion of these techniques is outside the scope of this chapter, and is included here only for completeness.
Risks
• Laceration of the vagina or puncture of the rectum are possible complications.
• As with all invasive procedures, there is the potential risk of bleeding or infection.
• Vaginal, retroperitoneal, and ischiorectal hematomas from damage to the pudendal artery, particularly with compromised coagulopathy, have been reported.19
• Although rare, systemic local anesthetic toxicity can occur. Symptoms could include: palpitations, dysarthria, tinnitus, drowsiness, confusion, convulsions, hypotension, bradycardia, and loss of consciousness.6
• Retropsoas or subgluteal infection is a possibility. Maintain a high titer of suspicion when there is back or hip pain and diminished range of motion postinjection.20
• Nerve injury or vascular injury may occur from the injection itself.
• Needle stick injuries to the physician with the associated risks of blood-borne pathogens, including HIV, may occur as the needle guide does not uniformly protect the physician.
POSTPROCEDURE FOLLOW-UP CONSIDERATIONS
• Because this injection is diagnostic as well as therapeutic, close monitoring of the immediate postprocedure analgesia is critical.
• Because the sciatic nerve is close to the pudendal nerve (Figure 62-12), there is a risk of leg weakness after the procedure.
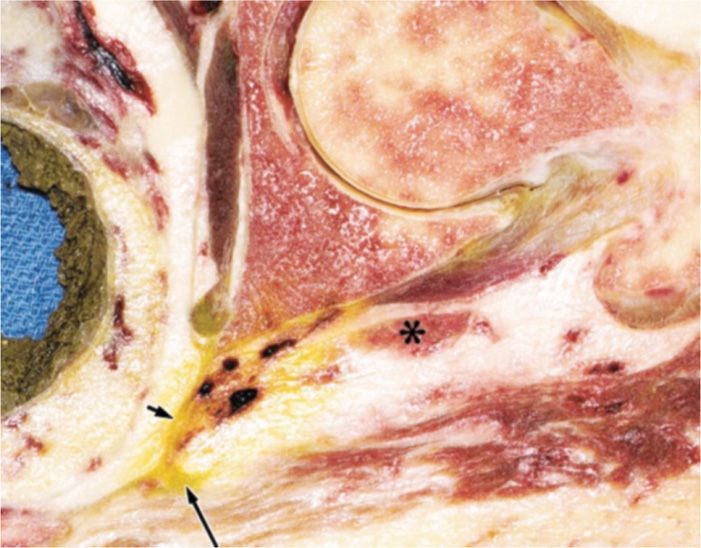
Figure 62-12. Pudendal injection. Arrow shows staining from pudendal injection; asterisk shows the sciatic nerve. (Reproduced with permission from American Journal of Roentgenology. Hough DM, Wittenberg KH, Pawlina W, et al. Chronic perineal pain caused by prudendal nerve entrapment: anatomy and CT-guided perineural injection technique. AJR Am J Roentgenol 2003; 181:561-7.)
MONITORING OF POTENTIAL COMPLICATIONS
2 types of complications
• Intraoperative
![]() Due to placement of the needle
Due to placement of the needle
![]() Needle injury to nerve, artery, surrounding tissues
Needle injury to nerve, artery, surrounding tissues
![]() Intravascular injection leading to toxic reaction
Intravascular injection leading to toxic reaction
![]() Monitor patient response during injection
Monitor patient response during injection
![]() Pain on injection or needle movement
Pain on injection or needle movement
![]() Complaints of agitation, palpitations, nausea
Complaints of agitation, palpitations, nausea
• Postoperative
![]() Bleeding, infection, steroid reaction
Bleeding, infection, steroid reaction
![]() Monitor patient for several days after procedure, looking for orthostatic blood pressure changes, fever, increased pain, personality changes, polyuria, muscle cramping
Monitor patient for several days after procedure, looking for orthostatic blood pressure changes, fever, increased pain, personality changes, polyuria, muscle cramping
CLINICAL PEARLS AND PITFALLS
• Treating patients with pelvic pain is a daunting task for many interventional pain physicians, and yet the pudendal nerve is very amenable to treatment.
• Diagnosis is made by a careful history (perineal pain, pain with sitting, history of trauma) and physical examination (tenderness at the ischium), followed by a diagnostic injection.
• Small volumes are necessary to avoid anesthetizing unexpected or unwanted structures.
• Pudendal nerve blocks at the ischial spine may help identify in general pain related to the pudendal nerve, but, since there are 2 potential sites of entrapment, injection at a distal entrapment site or both sites may be necessary to provide relief.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


