Algorithm for in-hospital resuscitation.
Cardiopulmonary resuscitation
Although cardiopulmonary resuscitation (CPR) is traditionally divided into basic life support (BLS) and advanced life support (ALS), this division is arbitrary when cardiac arrests occur in hospital. The immediate response will depend both on the skills of the initial rescuer and on the equipment available. The aim of effective CPR is to restore a spontaneous circulation to the patient as soon as possible. Although in most circumstances it is possible to support ventilation for prolonged periods effectively, there is no equivalent method of providing circulatory support without a heart beating in an effective rhythm producing cardiac output.
Basic life support
Basic life support (BLS), strictly defined, is the maintenance of a clear airway while supporting ventilation and circulation without the use of specialist equipment other than a protective airway device, e.g. a pocket mask. Current guidelines place a greater emphasis on good-quality chest compressions with minimal interruptions, as there is evidence that this is associated with improved survival.
The recommendation of a specific cardiac compression: ventilation ratio is a compromise between the need to generate forward blood flow and the need to supply oxygen to the lungs to optimise oxygen delivery to the brain and other vital organs. A 30:2 ratio is recommended, taking into account evidence available to optimise outcomes during CPR. The guidelines have been kept simple to aid learning and retention of BLS skills.
The adult BLS algorithm is as shown in Figure 8.3. Before approaching a collapsed person, a priority is to ensure both personal safety and that of bystanders. Although this is more important outside hospital, there are still safety issues to be considered within the hospital environment. Check for a response by shaking the person’s shoulders gently and asking loudly ‘are you alright?’ If there is no response, shout for help and turn the patient onto his or her back, except in pregnancy (see Resuscitation of the pregnant patient), and commence BLS.
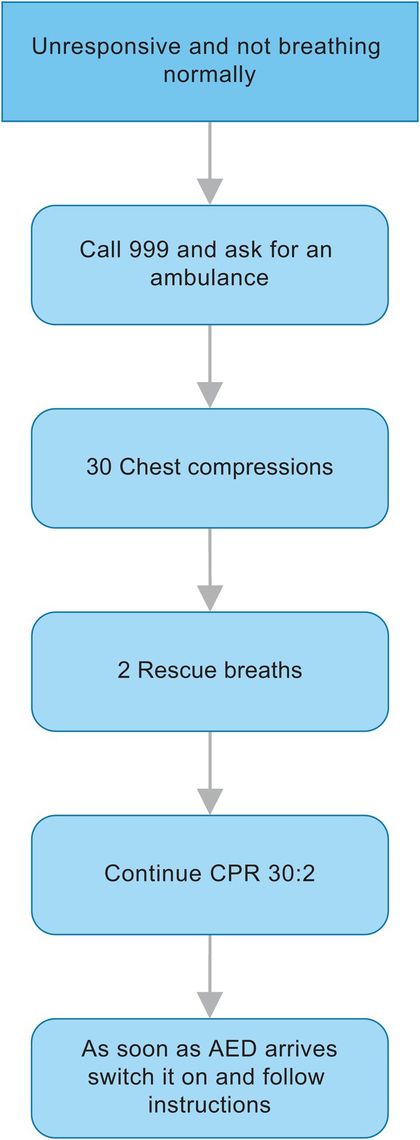
Adult basic life support (BLS) algorithm.
Airway
The maintenance of a patent airway during the management of a cardiorespiratory arrest is imperative. In an unconscious patient the tongue falls backwards and the airway is obstructed at the oropharyngeal level. Three simple airway manoeuvres, head tilt, chin lift and jaw thrust, can all be used to open the airway. In a patient who is still making respiratory effort, this may prevent the patient from deteriorating and suffering a cardiorespiratory arrest. The head tilt, which flexes the lower cervical spine while extending the head at the atlanto-occipital joint, and the chin lift may be sufficient to open an obstructed airway. If not, a jaw thrust may be added to further displace the tongue forwards.
In trauma cases where there is a suspected cervical spine injury, manual in-line traction must be applied and jaw-thrust/chin-lift techniques used to open the airway. If still unable to adequately clear the airway, a gentle head tilt may be added. Although all these airway manoeuvres are associated with some cervical spine movement, the maintenance of an open airway is the overriding priority and damage to spinal cord from excessive head tilt has never been reported in cases where cervical spine injury has been suspected.
Look in the mouth to check for any obvious obstruction and use a finger sweep to clear any visible foreign body present within the oropharynx. Then, taking no longer than 10 seconds, look for chest moments, listen for breath sounds, and feel for air movement. If the respiratory pattern is not normal and the patient is unresponsive, call for help and start cardiac compressions.
Circulation
Chest compressions must be started with the patient placed in a supine position on a firm surface. The correct hand position for cardiac compressions is found by placing the heel of the dominant hand in the centre of the chest between the nipples. The heel of other hand is then placed on top and the fingers interlocked, ensuring that pressure is applied over the sternum and not the ribs or abdomen. The rescuer assumes a position vertically above the patient’s chest and with straight arms applies compressions to a depth of 5–6 centimetres and at a rate of 100–120 compressions per minute.
The time taken for compression and release should be equal. After each compression all pressure on the chest must be released without losing contact between hands and sternum. If chest recoil is not complete it may lead to significantly increased intrathoracic pressure, decreased venous return and decreased coronary and cerebral perfusion.
Properly executed cardiac compressions are tiring, and there is evidence that the quality of chest compressions deteriorates as the rescuer tires. If there is more than one rescuer present, change the person performing cardiac compressions every 2 minutes.
Cardiac compressions generate forward blood flow by increasing intrathoracic pressure and directly compressing the heart. Although the mean carotid arterial pressure, even with good-quality cardiac compressions, seldom exceeds 40 mmHg, it provides a small but critical blood flow to the brain and myocardium.
During a VF arrest, blood continues to flow into and dilate the right ventricle. Early CPR prevents the right ventricle dilating and thereby increases the likelihood that a defibrillatory shock will terminate VF and enable the heart to resume an effective rhythm. It may also prevent an initial rhythm of VF deteriorating to asystole. With evidence that a patient stands the best chance of survival if rapidly resuscitated from VF, automated external defibrillators (AED) are being introduced widely in public places as well as becoming standard equipment on many hospital wards. For in-hospital cardiac arrests the use of an AED is an integral part of BLS.
Allowance has now been made in the guidelines for the rescuer who is unable or unwilling to perform mouth-to-mouth ventilation. Chest compressions alone are recommended in this situation. This will only be effective for the first few minutes, and then only in cases of non-hypoxic cardiac arrests, as within 4–6 minutes all oxygen stores are depleted. It is not recommended as standard management.
Rescue breathing
Expired air ventilation is the standard method used for rescue breathing in BLS, and produces an inspired oxygen content of 16–17%. Using chin-lift/head-tilt and/or jaw-thrust manoeuvres, the airway is opened while the rescuer takes a normal breath. If a pocket mask is not readily available, the soft part of the nose is closed by pinching between the index finger and thumb and the rescuer’s lips are placed round the patient’s mouth, making sure that a good seal is achieved before expiration. As well as mouth-to-mouth and mouth-to-nose ventilation, if the mouth is clenched shut or is badly injured, mouth-to-tracheal stoma ventilation is effective. The chest must be observed to rise and fall during each rescue breath.
Each rescue breath is given over 1 second, at a rate of 10–12 breaths per minute, to produce tidal volumes of about 500 mL. This limits interruptions to cardiac compressions and minimises gastric distension. Gastric distension splints the diaphragm and interferes with ventilation as well as increasing the risk of aspiration. Large tidal volumes increase intrathoracic pressure, decreasing coronary and cerebral perfusion, and in animals have been shown to reduce the chance of successful return of spontaneous circulation. Oxygenation is not impaired by the use of small tidal volumes, and the resulting hypercarbia and acidosis has not been shown to adversely affect outcome. The time taken to give two rescue breaths should be less than 5 seconds, which limits interruptions to cardiac compressions.
Only stop resuscitation if there are signs of regaining consciousness such as coughing, opening eyes, speaking or moving purposefully and there is resumption of normal respiration. Once cardiac output and normal respiration have been re-established, the patient should be turned into the recovery position. This is a stable lateral position, with the head dependent and no pressure on the chest to impair breathing. With increasing levels of obesity, the risks of injury to the rescuer when turning the patient must be balanced against the risks associated with leaving the patient supine.
Special situations
Foreign-body airway obstruction
Choking in adults tends to occur when eating, and should be promptly recognised and treated. If not, and the airway is severely compromised, the victim’s condition will rapidly deteriorate to a cardiorespiratory arrest. If there is mild respiratory distress, characterised by the ability to speak, breathe and cough, the victim should be encouraged to cough to clear the obstruction.
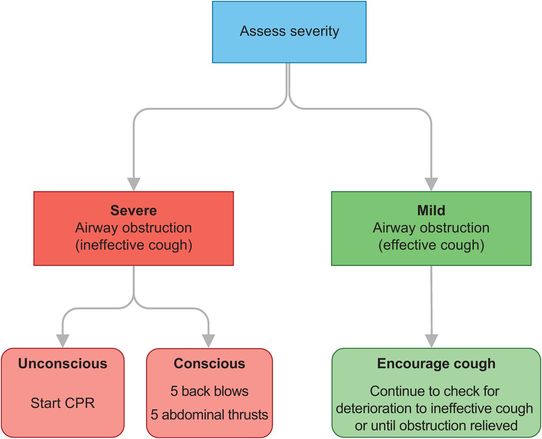
Adult choking algorithm.
If there is severe airway obstruction, the victim will be unable to speak, breathe or cough. If the victim remains conscious, stand to one side slightly behind them and, while supporting the chest with one hand, lean the victim forwards so that the obstructing object when dislodged comes out of the mouth. Immediately give up to five back blows between the shoulder blades with the heel of your hand. The aim is to dislodge the foreign body with each blow, rather than to give all five.
If this fails to relieve the airway obstruction, give up to five abdominal thrusts. Stand behind the victim, with both arms around the upper part of the abdomen, between the umbilicus and xiphisternum. Clench your fist and, while holding this with your other hand, pull sharply inwards and upwards. Repeat the abdominal thrust manoeuvre up to five times. There is no evidence to suggest which method should be used first. If the obstruction is still not relieved, continue alternating five back blows with five abdominal thrusts.
If the patient is initially unconscious or loses consciousness at any time, call for help and start BLS (Figure 8.3).
Advanced life support
Advanced life support (ALS) is a continuum of BLS and involves the use of extra equipment to aid resuscitation attempts. The adult ALS algorithm (Figure 8.5) provides a standardised approach to the treatment of all adult patients presenting in cardiac arrest.
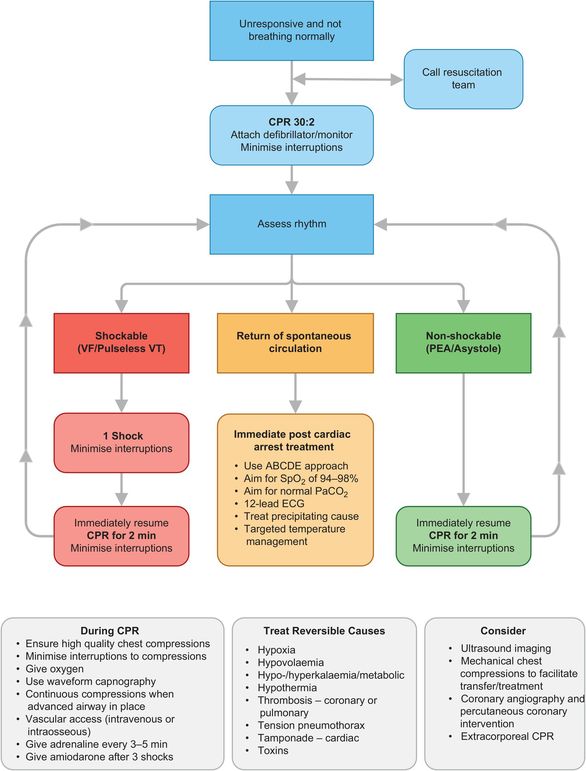
Adult advanced life support (ALS) algorithm.
Arrhythmias associated with a cardiac arrest are divided into two groups: shockable rhythms (ventricular fibrillation (VF) and ventricular tachycardia (VT)) and non-shockable rhythms (asystole and pulseless electrical activity (PEA)). The main difference in the management of these arrhythmias is the need for early defibrillation in patients with VF/VT. Subsequent actions, including advanced airway management, ventilation, good-quality chest compressions, venous access and administration of adrenaline, are common to both groups.
During CPR it is imperative that repeated attempts are made to identify and treat potentially reversible causes (Figure 8.5).
Airway
Even when correctly performed by experienced personnel, the simple airway manoeuvres as taught in BLS do not always allow maintenance of a clear airway. The use of mechanical aids should help, but if these are used by inadequately trained personnel there may be increased complications without any improvement in airway management.
Forceps or suction are used to remove any foreign material visible in the oropharynx.
Pharyngeal airways, inserted by either the oral or the nasal route, overcome the backward displacement of the soft palate and tongue. The oropharyngeal airway can only be used in unconscious patients and must be removed if there is gagging or retching. The nasopharyngeal airway is useful in situations where the mouth cannot be opened, but must be inserted gently as there is a risk of haemorrhage. In most cases the benefit of improved airway patency outweighs this risk.
A laryngeal mask airway (LMA) or iGel is relatively easy to insert and provides more efficient ventilation than standard bag-mask ventilation. Cardiac compressions may still need to be interrupted to enable adequate ventilation without an excessive air leak. The LMA only offers partial airway protection during CPR, but there have been few case reports of aspiration in this situation.
Endotracheal intubation remains the gold standard in airway management during CPR. Its use protects the airway from aspiration, prevents gastric distension, allows suction of airway secretions, provides a route for drug administration and allows cardiac compressions to continue uninterrupted during ventilation. Disadvantages include a comparatively high failure rate when performed by non-anaesthetists, the risk of a misplaced tube, and prolonged periods of time without cardiac compressions while attempts are made to intubate. Endotracheal intubation should therefore only be attempted by trained personnel, taking no longer than 10 seconds to complete the process, in order to minimise interruptions to cardiac compressions. Correct placement of the endotracheal tube must be confirmed, as with intubation in theatre. The 2015 guidelines for ALS recommend the use of capnography to both confirm and continually monitor tube placement. An increase in end-tidal carbon dioxide concentrations may provide an early indication of the return of a spontaneous circulation.
A needle or surgical cricothyroidotomy can be life-saving in the ‘can’t intubate, can’t ventilate’ scenario when there is extensive facial trauma or laryngeal obstruction secondary to oedema or foreign-body ingestion. Percutaneous or surgical tracheostomies are not recommended in this emergency situation, as they take too long to perform.
Ventilation
As in BLS, inspiratory time for ventilation should be limited to 1 second, producing a tidal volume of about 500 mL at a rate of 10–12 breaths per minute. This allows adequate ventilation without excessive interruptions to cardiac compressions. Although expired air ventilation provides effective ventilation, an inspired oxygen concentration of only 16–17% can be achieved. A self-inflating bag will deliver 21% oxygen, and this can be increased to 45% if oxygen is attached directly to the bag. With the addition of a reservoir system and oxygen at 15 L per minute, an inspired oxygen concentration exceeding 85% can be achieved.
To effectively ventilate a patient with a bag-mask technique is difficult, and meticulous attention must be paid to maintaining an open airway while observing the rise and fall of the chest. Even when skilled in airway management, bag-mask ventilation is often a two-person technique. Endotracheal intubation will in most cases, and the use of a LMA may, allow ventilation at a rate of 10 breaths per minute, without interruptions of cardiac compressions.
Circulation
When an unmonitored patient suffers a cardiac arrest, initial attention should be focused on providing good-quality minimally interrupted chest compressions as described for BLS (cardiac compressions : ventilation ratio 30:2). Chest compressions should only be briefly paused to allow a specific intervention to take place. As soon as a defibrillator arrives the cardiac rhythm must be monitored and the appropriate limb of the ALS algorithm (Figure 8.5) followed, depending on the diagnosis.
Shockable rhythms (VF/VT)
The most common presenting rhythm at a cardiac arrest is VF, and if VF is present for more than a few minutes the myocardium is depleted of oxygen and metabolic substrates. A brief period of chest compressions before defibrillation will deliver small amounts of oxygen and energy substrates, which will increase the probability of restoring a perfusing rhythm after shock delivery. Early defibrillation has been shown to improve the chances of survival in VF/VT arrests.
Once VF or pulseless VT has been diagnosed, defibrillation should be attempted as soon as possible. Shock energies should start at 150 J and may be repeated or increase with subsequent shocks to a maximum of 360 J. Chest compressions should continue while the defibrillator is charged to minimise the pre-shock pause. CPR should resume immediately after the first shock and continue for 2 minutes before reassessing the rhythm. If VT/VF persists, give a second shock and restart CPR immediately. Continue for a further 2 minutes before pausing to reassess the rhythm and, if still in VT/VF, give a third shock, resume CPR, and give adrenaline, 1 mg IV, and amiodarone, 300 mg IV. Continue the 2-minute CPR, rhythm/pulse check, defibrillation sequence, and if VF/VT persists, on alternate cycles give adrenaline 1 mg IV immediately following shocks (approximately every 3–5 minutes).
If at any time organised electrical activity is seen when checking the rhythm, and there are no clinical signs of spontaneous circulation (i.e. signs of regaining consciousness such as coughing, opening eyes, speaking or moving purposefully, normal respiration, or increasing end-tidal carbon dioxide concentrations on capnography), change to the non-shockable limb of the algorithm; similarly if the rhythm deteriorates to asystole.
Fine VF is very difficult to distinguish from asystole, and is unlikely to be shocked into a perfusing rhythm. Repeated attempts at defibrillation not only cause myocardial damage but also repeatedly interrupt chest compressions. If fine VF is suspected start CPR, which may increase the amplitude and frequency of VF and the chances of successful defibrillation.
A precordial thump is now recommended only in the case of a witnessed cardiac arrest when a defibrillator is not immediately available. Although a precordial thump may convert VT to sinus rhythm, and has been reported to convert VF into sinus rhythm if given within 10 seconds of a VF arrest, rare adverse effects have also been reported. These include rate acceleration of VT, conversion of VT to VF, complete heart block and asystole.
A precordial thump is performed by using the ulnar edge of a tightly clenched fist to deliver a sharp impact to the lower half of the sternum from a height of about 20 cm. The fist should immediately be retracted to create an impulse-like stimulus. The mechanical energy of the thump is converted to electrical energy, which may be sufficient to achieve defibrillation.
Electrical defibrillation
Electrical defibrillation is the passage of an electrical current across the myocardium that is of sufficient magnitude to depolarise a critical mass of myocardium. If the heart is still viable, normal pacemakers will take over and produce coordinated electrical activity, which will restore spontaneous circulation. The optimum energy to use is that which achieves defibrillation of a critical mass of myocardium while causing minimal myocardial damage. Transthoracic impedance, typically 70–80 Ω in adults, is at its lowest at the end of expiration, and defibrillation should be attempted at this point of the respiratory cycle. Shaving a hairy chest may also further reduce impedance by improving contact between pad/paddle and skin.
Self-adhesive pads are preferred to manual paddles as they not only allow delivery of shocks more rapidly and defibrillation from a safe distance, but also facilitate continuation of chest compressions during charging of the defibrillator. Pads or paddles can be placed in the anteroapical position, with the right sternal pad to the right of the sternum below the clavicle and the apical pad in the mid-axillary line in the V6 ECG electrode position. An alternative position is to place pads/paddles anteroposteriorly, which may provide more effective defibrillation. However, this must be balanced against the difficulty in applying the posterior pad/paddle to an unconscious patient. If there is a pacemaker or implantable cardioverter defibrillator (ICD) present, it is safer to place the pads away from the device if possible.
ALS guidelines advise a single-shock protocol (Figure 8.5), and not three stacked shocks as previously recommended. The stacked-shock protocol led to significant periods of time without cardiac compressions, which has been shown to be detrimental to a patient’s chance of survival. Defibrillator technology has also advanced, producing biphasic waveforms, which are more efficient than the monophasic waveforms produced by older defibrillators. The success of the first shock from a biphasic defibrillator now exceeds 90%, and failure to terminate VF/VT indicates the need for further CPR to improve myocardial oxygenation rather than the need for further shocks. Biphasic devices produce either truncated exponential waveforms or rectilinear biphasic waveforms, and these require different energy levels for defibrillation. Manufacturers should display an effective waveform energy range on the biphasic device, but if unsure use 200 J for the first shock.
Even if defibrillation is successful, it is very rare for a pulse to become palpable immediately after defibrillation, and CPR must therefore be restarted immediately after delivery of a shock. If a perfusing rhythm has not been restored, this avoids a further interruption of CPR. If a perfusing rhythm has been restored, CPR is not detrimental and will not precipitate further episodes of VF/VT. If the shock has converted VF/VT into asystole, then a further period of CPR may induce VF, which has a better prognosis.
Non-shockable rhythms (pulseless electrical activity and asystole)
Pulseless electrical activity (PEA) is when cardiac electrical activity is present but there are no palpable pulses. A PEA arrest resulting from primary myocardial pump failure carries a very poor prognosis; however, it is often secondary to potentially reversible causes listed in Figure 8.5, and if these are rapidly identified and appropriately treated, PEA is often survivable.
When PEA is diagnosed CPR must be started immediately according to the ALS algorithm, and when IV access is achieved 1 mg of adrenaline (IV) should be given. Continue CPR at a ratio of 30:2 until the airway is secured with an endotracheal tube, and then continue cardiac compressions uninterrupted with a ventilation rate of 10–12 breaths per minute. After 2 minutes of CPR recheck the rhythm, and if an organised rhythm is present also check for a pulse. If PEA persists, continue with 2-minute cycles of CPR, giving further adrenaline 1 mg IV on alternate cycles (every 3–5 minutes). Repeated attempts should be made to identify and treat any potentially reversible causes.
As soon as asystole is diagnosed start CPR immediately. While continuing CPR, check that all monitoring devices are correctly attached and that there is not a disconnection producing an apparent asystolic trace. Establish IV access, give 1 mg of adrenaline (IV), and continue with CPR for 2 minutes, before rechecking the rhythm. If asystole persists, the airway should be secured and CPR continued in accordance with the ALS algorithm (Figure 8.5). Adrenaline (1 mg IV boluses) should be given every 3–5 minutes. During rhythm checks the ECG should be carefully scrutinised for the presence of P waves: if present, pacing may restore a perfusing rhythm.
If at any time the rhythm changes to VF/VT then the shockable limb of the ALS algorithm should be followed.
Drug usage
The most common route for drug administration during a cardiorespiratory arrest is via a peripheral IV cannula. It is relatively quick and easy to establish, when compared with central venous access, and is safer. When drugs are given peripherally each dose should be flushed with 10–20 mL of saline and the limb elevated for 10–20 seconds to facilitate drug delivery. If a central venous line is present it should be used in preference to peripheral lines, as higher peak drug concentrations are achieved and drug circulation times are shorter. However, to insert a central venous line at the time of a cardiac arrest is time-consuming, which necessitates time without chest compressions, and is associated with a high risk of complications.
It is now recommended that if intravenous access has not been established within 2 minutes, the intraosseous (IO) route should be considered in adults as well as in children. With the ease of gaining IO access using semi-automated devices and the knowledge that plasma concentrations achieved from tracheal administration of drugs are variable and unpredictable, giving drugs via the endotracheal tube is no longer recommended.
Adrenaline
Adrenaline 1 mg IV remains the vasopressor of choice in all forms of cardiac arrest. It has potent α effects, causing widespread vasoconstriction, which increases coronary and cerebral perfusion pressure, and β-adrenergic effects, which increase coronary and cerebral blood flow through inotropic and chronotropic actions. However, some of these beneficial β-effects may be offset by increased myocardial oxygen consumption and increased ventricular arrhythmogenicity. Although its use is still recommended, there remains no good evidence which shows that the use of any vasopressor at any stage during CPR increases neurologically intact survival.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


