CHAPTER 9 Preoperative Preparation
In addition to having a sound understanding of a child’s medical disease and anticipated surgical procedure, the anesthesiologist must also appreciate the emotional stresses that affect both the child and parent. The preoperative meeting with the patient and his or her parents is not only a responsibility of the anesthesiologist but also an important opportunity to learn facts that could otherwise be missed. It is a chance to win the confidence of the patient and the parents, if they are present (Fig. 9-1).
A careful preoperative examination of the child and the child’s medical record enables the anesthesiologist to assess the child’s general state of health and to identify the presence of chronic, acute, or intercurrent diseases, as well as to recognize previous anesthetic problems (Black, 1999). From this knowledge, appropriate subspecialty consultation can be sought, the operative medical condition can be optimized for the surgery, and the anesthetic plans can be made. In addition to monitoring practices and anesthetic techniques, anesthetic plans should include provisions for the patient’s postoperative care, particularly an analgesic plan. It is the general goal of the preanesthetic visit to anticipate potential complications before they occur, to avert them when possible, and, in so doing, to minimize the risks to the health of the child. The risk of anesthesia is assessed during the preoperative visit, and the child’s parents should be informed of the plans for anesthesia and monitoring, and they should be apprised of the anticipated risk.
Preanesthetic Visit
The preanesthetic visit should begin with a careful review of the medical record; particular attention should be paid to previous anesthetic agents and problems encountered, the successful and unsuccessful techniques used in the past for airway management, and any history of cardiorespiratory diseases or airway anomalies. A history of medical or environmental allergies should be elicited, and it should include questions specifically directed toward evaluating the presence of allergy to latex in children at risk, notably those with meningomyelocele or urogenital anomalies, those who undergo bladder self-catheterization, or those whose medical histories indicate a significant amount of latex exposure in the past (Holzman 1997; Porri et al., 1997; Hollnberger et al., 2002; Pires et al., 2002; Eustachio et al., 2003; Dehlink et al., 2009; Rendeli et al., 2006; Bostancy et al., 2007; Dieguez et al., 2007; Garcia 2007; Baker and Hourihane, 2008; De Queiroz et al., 2009). Results of laboratory tests should be reviewed, focusing on hematologic evaluations, renal function, and electrolyte profiles, as well as blood gas analysis and pulmonary function tests when appropriate.
The anesthesiologist must be aware of the child’s current drug therapy and how it may interact with the anesthetic. The perioperative administration of bronchodilators, cancer chemotherapeutic agents, or anticholinesterases has significant implications for anesthesia (Schein and Winoker, 1975; Selvin, 1981; Drummond, 1984). Corticosteroid administration is traditionally recommended for patients who receive chronic corticosteroid therapy and for patients who have received steroids in the past, although evidence for the necessity of doing so is lacking (see Chapter 36, Systemic Disorders). Current drug therapy must also include questions regarding the use of herbal medications. Potential complications in the perioperative period have been attributed to the use of complementary medicines. Table 9-1 summarizes the most commonly used herbal remedies (Ang-lee et al., 2001).
TABLE 9-1 Pharmacologic Effects and Potential Perioperative Complications of Eight Commonly Used Herbal Remedies
| Name of Herb | Common Uses | Potential Perioperative Complications |
| Echinacea, purple cone flower root | Prophylaxis and treatment of viral, bacterial, and fungal infections | Reduced effectiveness of immunosuppressants; potential for wound infection; may cause hepatotoxicity when used with other hepatotoxic drugs |
| Ephedra, ma-huang | Diet aid | Dose-dependent increase in heart rate and blood pressure; arrhythmias with halothane; tachyphylaxis with intraoperative ephedrine |
| Garlic, ajo | Antihypertensive, lipid-lowering agent, anti-thrombus forming | May potentiate other platelet inhibitors; perioperative bleeding |
| Ginkgo, maidenhair; fossil tree | Circulatory stimulant; Alzheimer’s disease, peripheral vascular disease, and erectile dysfunction | May potentiate other platelet inhibitors; perioperative bleeding |
| Ginseng | To protect the body against stress and restore homeostasis | Perioperative bleeding; potential for hypoglycemia |
| Kavakava, pepper | Anxiolytic | Potentiates sedative effects of anesthetic agents; possible withdrawal syndrome after sudden abstinence; kavakava-induced hepatotoxicity |
| St. John’s wort, goatweek, amber, hardhay | Treatment for depression and anxiety | Decreased effectiveness of cyclosporine, alfentanil, midazolam, lidocaine, calcium channel blockers, and digoxin |
| Valerian, vandal root, all heal | Anxiolytic and sleep aid | Potentiates sedative effects of anesthetic agents; withdrawal-type syndrome with sudden abstinence |
From Skinner CM, Rangasami J: Preoperative use of herbal medicines: a patient survey, Br J Anaesth 89:792-795, 2002.
Many unusual syndromes occur in childhood, and they often have multisystem involvement; consequently, they have an important impact on anesthetic management. An important caveat in pediatric medicine is that when one congenital anomaly exists, there is a significant likelihood of anomalies involving other organs. For example, infants with tracheoesophageal fistulas have an increased incidence of congenital heart disease, and some forms of radial dysplasia are associated with thrombocytopenia or atrial septal defects. The topic of congenital anomalies was extensively discussed in a review by Lynn (1985). The remainder of this section is a review of pediatric diseases that may be important to the anesthesiologist. Information regarding these problems may be forthcoming from the child’s medical history, the physical examination, or both.
Physical Examination
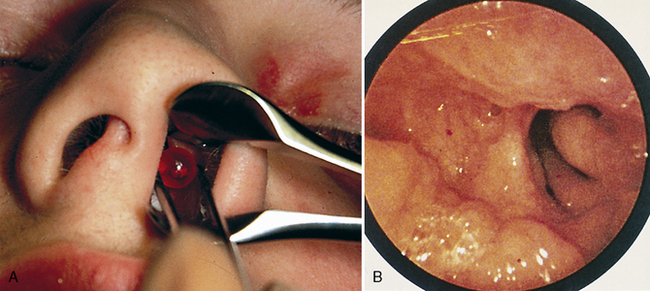
Partial airway obstruction may result from infection, anatomic anomalies, or tumors. When possible, a diagnosis should be made before anesthesia is begun. Unilateral nasal discharge is unusual and suggests a foreign body (or, less often, choanal atresia) (Fig. 9-2).
Review of Body Systems (Table 9-2)
Central Nervous System
TABLE 9-2 Medical History and Review of Systems: Anesthetic Implications
| System | History | Potential Anesthetic Implication |
| Central nervous and neuromuscular systems | Seizure Head trauma Hydrocephalus Central nervous system tumor Developmental delay Neuromuscular disease Muscle disease | Medications: drug interactions, inadequate anticonvulsant therapy, drug-induced hepatopathology Elevated intracranial pressure Anemia Elevated intracranial pressure Elevated intracranial pressure Chemotherapeutic drug interactions History of steroid useBulbar dysfunction Risk of aspiration Altered response to relaxants Risk of malignant hyperthermia Risk of rhabdomyolysis and hyperkalemia |
| Cardiovascular system | Heart murmur Cyanotic heart defect History of squatting Diaphoresis with feeding or crying Hypertension | Risk of right-to-left air embolism of intravenous air bubbles Need for SBE prophylaxis Right-to-left cardiac shunt Risk of right-to-left air embolism of intravenous air bubbles Hemoconcentration Need for SBE prophylaxis Teratology of Fallot Congestive heart failure Coarctation of the aorta, renal disease, or pheochromacytoma |
| Respiratory system | Prematurity Bronchopulmonary dysplasia Respiratory infection, cough Croup Snoring Asthma Cystic fibrosis | Increased risk of postoperative apneaLower airway obstruction Reactive airways disease Subglottic stenosis Pulmonary hypertension Reactive airways and bronchospasm Medication history Subglottic stenosis or anomaly Obstructive sleep apnea Perioperative airway obstructionβ-Agonist or theophylline therapy History of steroid useDrug interactions Pulmonary toilet Pulmonary dysfunction and VQ mismatch Reactive airways disease |
| Gastrointestinal/hepatic systems | Vomiting, diarrhea Growth failure Gastroesophageal reflux JaundiceLiver transplant recipient | Electrolyte abnormality, especially hypokalemia Dehydration Risk of aspiration Low glycogen reserves/risk of hypoglycemia AnemiaRisk of aspiration Reactive airways disease Anemia Altered drug metabolism Risk of hypoglycemia Coagulopathy Altered drug metabolism Immunosuppression Coagulopathy |
| Renal system | Frequency, nocturia Renal failure/dialysis Kidney transplant recipient | Occult diabetes mellitus Electrolyte disturbance Urinary sepsis Electrolyte disturbance Hypervolemia or hypovolemia Anemia Medication history Immunosuppression Poor toleration of hypotension Hypertension |
| Endocrine system | Diabetes Steroid therapy | Insulin requirement Intraoperative hyperglycemia or hypoglycemia Adrenocorticoid suppression |
| Genitourinary system | Pregnancy | Teratogenic effects Risk of spontaneous abortion |
| Hematologic system | Anemia Bruising, history of bleeding Sickle cell disease Human immunodeficiency virus infection | Transfusion requirement Occult hemoglobinopathy Coagulopathy Anemia Need for hydration Limb tourniquet use Susceptibility to infection Infectious risk to medical personnel |
| Dental system | Loose primary teeth | Risk of aspiration if tooth avulsed |
SBE, Subacute bacterial endocarditis; VQ, ventilation perfusion.
Modified from Coté CJ, Todres ID, Ryan JF: Preoperative evaluation of pediatric patients. In Ryan JF, Todres ID, Coté CJ, et al., editors: A practice of anesthesia for infants and children, New York, 1986, Grune & Stratton. (With permission from Elsevier.)
Trauma is the most common cause of death in children, and most fatal trauma involves injury to the CNS. Head injuries often result in an altered level of consciousness, cerebral edema, and elevated intracranial pressure. Tumors of the brain are the most common solid tumors of childhood and usually occur in the posterior fossa. They generally increase intracranial pressure as a mass effect but also often obstruct cerebrospinal fluid pathways, resulting in hydrocephalus. The anesthetic care of children with elevated intracranial pressure is discussed in Chapter 22, Anesthesia for Neurosurgery.
Neuromuscular diseases, such as congenital myotonia, muscular dystrophy, and the various forms of myositis, contraindicate the use of succinylcholine even in emergency airway management, although it is rarely used in current pediatric anesthetic practice (see Chapter 36, Systemic Disorders). In myotonia, succinylcholine produces a sustained contracture of skeletal muscle that may impede the ability to maintain a patent airway and ventilate the lungs. In other myopathies, such as clinically active dermatomyositis, succinylcholine produces life-threatening hyperkalemia. Some forms of muscular dystrophy (central core disease) are statistically associated with malignant hyperthermia, whereas others may result in a malignant hyperthermia-like syndrome that is equally life threatening (Guis et al., 2004; Rosenberg et al., 2007; Driessen and Snoeck, 2008; Hayes et al., 2008; Puel et al., 2008; Takagi and Nakase, 2008; Schwartz and Raghunathan, 2009). Although not all children with Duchenne’s or other muscular dystrophies are genetically susceptible, Rosenberg and Heiman-Patterson (1983), as well as Takagi and Nakase (2008), recommend that precautions against malignant hyperthermia be taken in patients with this disorder because of rhabdomyolysis and hypermetabolism that may occur in myopathic children after exposure to triggering agents. For further discussion please refer to Chapter 37, Malignant Hyperthermia.
Cardiovascular System
Asymptomatic cardiac murmurs occasionally have implications for anesthesia. If they represent small ventricular septal defects or mild valvular disease, prophylaxis against bacterial endocarditis is indicated for procedures that may result in bacteremia, such as dental surgery, gastrointestinal or urogenital endoscopy, and nasotracheal intubation (Wilson et al., 2007). Atrial septal defects contraindicate the use of the sitting position for suboccipital craniotomies in order to minimize the risk of paradoxical air embolism (Fischler, 1992). The defects may also make intraoperative transesophageal echocardiography desirable in certain cases that have been associated with venous air embolism (e.g., posterior spine fusions or liver transplantation), so the movement of air from the pulmonary to the systemic circulation may be detected. If the anesthesiologist detects a previously undescribed murmur in these circumstances, a consultation with the cardiologist is indicated to further delineate the nature of the lesion (Fig. 9-3). Many congenital anomalies and syndromes are associated with cardiac defects or other cardiovascular problems; Box 9-1 provides an outline of these conditions.
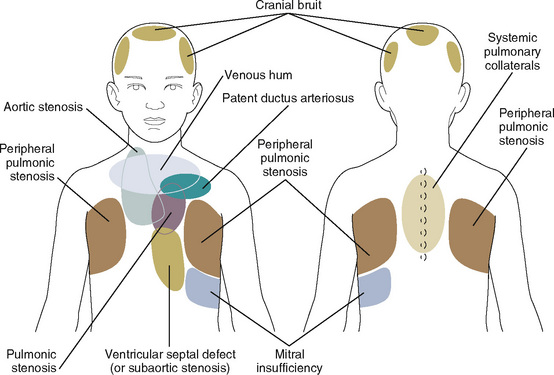
FIGURE 9-3 Sites for auscultation where murmurs are heard best.
(From Beerman LB, Kreutzer J, Park SC: Cardiology. In Zitelli J, Davis HW, editors: Atlas of pediatric physical diagnosis, ed 5, St Louis, 2007, Mosby.)
Box 9-1 Pediatric Syndromes Associated with Cardiac Conditions
Syndromes Associated With Congenital Heart Disease
Respiratory System
Chapter 3, Respiratory Physiology in Infants and Children, describes the anatomic and physiologic differences between the pediatric and adult respiratory systems. The differences in dimension and function predispose the child to perioperative airway obstruction, which mandates a critical preoperative evaluation of the airway. The upper airway of the child may be further compromised by many entities, including: tonsillar or adenoidal hypertrophy or both; craniofacial anomalies such as Crouzon’s disease, Apert’s syndrome, hemifacial microsomia, Goldenhar’s syndrome, Treacher Collins syndrome (or Pierre Robin syndrome); lingular hypertrophy (common in trisomy 21); Beckwith’s syndrome and the various forms of mucopolysaccharidosis (Hurler’s syndrome and Hunter’s syndrome being the most common); isolated airway anomalies, such as cleft palate, laryngeal web or cleft, laryngomalacia, or subglottic stenosis; or tumors, such as hemangiomas and lymphangiomas, which may occur anywhere along the airway. Cutaneous cervicofacial hemangiomas along a beard distribution are suggestive of an association with upper airway or subglottic hemangiomas (Orlo et al., 1997).
Acute upper respiratory tract infections provide a common dilemma for the anesthesiologist. The mere volume of publications that evaluate the risk of adverse events of anesthesia in children with upper airway infections speaks to the ongoing controversy (Tait and Malviya, 2005). In the best of all worlds, no child would be anesthetized electively during an acute respiratory illness. Although not all studies have identified acute respiratory illness as a cause of perioperative complications in children, there is compelling evidence that the occurrence of both intraoperative and postoperative hypoxemia and other airway complications are increased in children with upper respiratory tract infections (DeSoto et al., 1988; Cohen and Cameron, 1991; Kinouchi et al., 1992; Levy et al., 1992; Rolf and Coté, 1992; Parnis et al., 2001; Bordet et al., 2002; Elwood et al., 2003; Tait, 2005). There is also evidence that the incidence of bronchospasm is increased in the presence of upper respiratory infections in children who are intubated (Rolf and Coté, 1992; Rachel Homer et al., 2007; von Ungern-Sternberg et al., 2007). In a prospective study, Tait and colleagues (2001) noted that endotracheal intubation, a history of prematurity, reactive airways disease, parental smoking, airway surgery, and nasal congestion are all risk factors associated with respiratory complications in infants and children who have upper respiratory infections and who are undergoing anesthesia. Furthermore, the child with an acute respiratory disease exposes other patients and health care workers to their contagion, which may not be a trivial concern when these individuals are immunocompromised.
Other considerations, however, must be taken into account before making the decision to postpone surgery. For example, the relatively small risk to the child must be weighed against the expense and effort the family has made to come to the hospital, often from a distant locale and at the cost of lost income. Some children, particularly those seen for otolaryngologic surgery, appear to never be free from respiratory infections during much of the year. Postponement of surgery may not be practical in these circumstances. Indeed, one study indicates that myringotomy is therapeutic in these children and is not associated with an increased incidence of postoperative pulmonary complications (Tait and Knight, 1987).
Chronic diseases of the lower respiratory tract occur in both children and adults. Asthma and cystic fibrosis are the most common chronic pulmonary diseases of childhood. A careful history and physical examination usually suffice in the preoperative evaluation of these diseases. If preoperative impairment is severe, however, or if the planned surgery is extensive, formal pulmonology consultation and pulmonary function testing may provide the anesthesiologist with information that can be used to provide optimal postoperative care. Children with asthma are commonly medicated with β2-adrenergic agents and inhaled corticosteroids. Other first-line drugs include cromolyn sodium and leukotriene receptor antagonists; rarely are theophylline preparations administered at this time. However, when theophylline is a part of the patient’s treatment, serum concentration of theophylline should be measured preoperatively to ensure blood levels in a therapeutic range (10-20 mcg/mL), and the anesthesiologist should be aware of potential interactions among theophylline, β2-adrenergic drugs, and halothane (although it is not often used). Asthmatic children who receive corticosteroids should also be considered for perioperative therapy with stress doses of corticosteroids if steroid therapy has been recent, although as previously stated, the evidence to support this convention is lacking. For those children who have required systemic steroids in the past, a short course of steroids beginning 1 to 2 days before the day of surgery may be beneficial (see Chapter 36, Systemic Disorders).
Severe kyphoscoliosis typically leads to significant restrictive lung disease. This is particularly true in cases of kyphoscoliosis that occur before the teenage years. Particularly in this age group, the cause of the kyphoscoliosis should be assessed, because it typically results from neuromuscular diseases such as cerebral palsy or muscular dystrophy or from anatomic anomalies such as hemivertebrae, which may be part of a syndrome that is associated with other congenital anomalies of importance to the anesthesiologist (e.g., VATER association). Preoperative testing of pulmonary function may be useful in predicting which children will require admission to an intensive care unit with or without mechanical ventilation postoperatively, but usually the decision to mechanically ventilate patients after spinal surgery is based on general preoperative condition, duration and difficulty of surgery, blood loss, and other surgical factors, rather than on the test of pulmonary function itself (see Chapter 26, Anesthesia for Orthopedic Surgery).
An infant who was born prematurely is often left with a residual chronic obstructive pulmonary disease called bronchopulmonary dysplasia, the consequence of both oxygen toxicity and ventilator-induced lung injury to immature lungs. The incidence and severity of this disabling condition have been dramatically reduced by the use of surfactant in neonatal intensive care units. Children with bronchopulmonary dysplasia exhibit a combination of fibrotic and cystic changes in the lung parenchyma with reactive small airways disease, with or without wheezing and air trapping. These children may respond to steroids and bronchodilators in varying degrees. More advanced bronchopulmonary dysplasia is associated with chronic hypoxia, carbon dioxide retention, pulmonary hypertension, and ultimately cor pulmonale (Berman et al., 1982).
Life-threatening apnea and bradycardia may occur after general anesthesia, most commonly in the preterm infant who is still younger than 45 weeks’ or as old as 60 weeks’ postconceptional age (the sum of gestational age and postnatal age) (Liu et al., 1980; Kurth et al., 1986; Wellborn et al., 1986). Hospital admission and respiratory monitoring are necessary for infants at risk, even after brief general anesthesia. Risk factors for postoperative apnea in preterm infants include: a history of mechanical ventilation, history of apnea and bradycardia, and anemia at the time of surgery (Kurth and LeBard, 1991; Wellborn et al., 1991; Spear, 1992; Malviya et al., 1993; Coté et al., 1995). In a meta-analysis of eight studies, Coté et al. (1995) reported that the postconceptual age required to reduce the risk of postoperative apnea to 1% was 54 weeks for infants born at 35 weeks’ gestation and 56 weeks for infants born before 32 weeks’ gestation. For further information, see Chapter 17, Neonatology for Anesthesiologists, Figure 17-10.
Congenital diseases of the lungs are usually recognized and surgically corrected in the newborn period. These conditions and their anesthetic management are discussed in Chapters 18 and 23, Anesthesia for General Surgery in the Neonate, and Anesthesia for General Abdominal, Thoracic, Urologic, and Bariatric Surgery.
Renal System
Milder degrees of renal dysfunction may also affect anesthetic care. In small children with mild or moderate underlying renal disease, clinically significant hypervolemia may occur without compensation by augmented urine output, and an excessive sodium or free-water load further deranges the serum electrolyte level. Particular caution is important in the management of fluids in children, and central venous pressure monitoring is required during major surgery in which significant blood loss or fluid shifts are anticipated (see Chapter 5, Regulation of Fluids and Electrolytes).
Hematologic System
Underlying disorders of the hematologic system are not common. The systems review should include an inquiry into unusual bleeding in the family’s or child’s medical history to explore possible genetic coagulopathies. A report of excessive bleeding from a circumcision or tonsillectomy should raise the possibility of thrombocytopenia, von Willebrand’s disease, or one of the inherited factor deficiencies and is a reason to measure platelet count, bleeding time, and coagulation time (see Chapter 36, Systemic Disorders).
In a report by the Preoperative Transfusion in Sickle Cell Disease Study Group, aggressive treatment (transfusion to a hemoglobin S level of less than 30%) was compared with a more conservative management regimen (hemoglobin maintained at 10 g/dL). The conservative approach was equally as effective as the aggressive approach in preventing serious complications but was associated with half the number of transfusion-associated complications (Vichinsky et al., 1995). A hematologic consultation should be sought or institutional protocols be developed for children with hemoglobinopathies who are undergoing anesthesia (see Chapter 36, Systemic Disorders).









