Lower risk of pneumothorax than SCV
Low infection rates
Site of choice in obesity
Comfortable for patients
Useful in trauma or patients with spinal immobilization
Higher risk of pneumothorax – avoid in severe lung disease
Avoid in coagulopathy – unable to compress vessels easily
Venous stenosis – avoid in long-term dialysis patients
Good flow rates for dialysis lines
Good choice in the coagulopathic patient
No risk of pneumothorax
Higher thrombosis rate
Limits patient mobility
Approaches and landmarks
Internal jugular vein
Identify anatomy: carotid artery, thyroid cartilage, sternocleidomastoid muscle, clavicle
Insertion point:
High approach: medial border of sternal head of sternocleidomastoid, just lateral to the carotid artery at the level of the thyroid cartilage.
Middle approach: apex of triangle formed by the two heads of sternocleidomastoid muscle.
Low approach: posterior border of the sternal head of sternocleidomastoid muscle.
Direct the needle towards the ipsilateral nipple at an angle of 45°. The vein is usually very superficial and only 0.5–2 cm under the skin.
Tips and advice
Turn head to contralateral side, avoid excessive turning as it changes the relationship of the vein and artery and can collapse the vein.
If you experience difficulty in cannulating the vein or it keeps collapsing:
Make sure you are not compressing the vein too much with the USS probe or your fingers
Put the patient more head down
Consider giving a fluid bolus
Ask the patient to hold their breath or do a Valsalva manoeuver.
Subclavian vein
Identify anatomy: sternal notch and clavicle
Insertion point: 1 cm below the clavicle, at the junction of the medial third and middle third of the clavicle. Advance needle towards the sternal notch, guiding the needle under the clavicle. Some clinicians advocate identifying the clavicle initially by hitting it with the needle and then ‘walking’ the needle under the inferior border whilst keeping the needle as horizontal as possible to avoid the dome of the pleura.
Turn head to contralateral side.
Place a rolled up towel or bag of fluids between the scapula to extend the spine.
It you have difficulty locating the vein, ask an assistant to pull caudally on the ipsilateral arm.
If you are unable to get beneath the clavicle consider starting more laterally and bending your needle upward slightly.
If arterial puncture occurs, withdraw the needle and apply firm pressure both above and below the clavicle.
If a chest drain is already in situ (e.g. following chest trauma) place the CVC on the same side.
Femoral vein
Identify anatomy: inguinal ligament, femoral artery (the femoral vein lies medial to the artery)
Insertion point: palpate the femoral artery 2 cm below the inguinal ligament and insert the needle 1 cm medial to the pulsation and aim cephalad and slightly medially at an angle of 20–30° to the skin. In adults the vein is usually 2–4 cm below the skin.
Tips and advice
The patient should be supine with a pillow under the buttocks to elevate the groin. The thigh should be abducted and externally rotated.
It can be difficult to feel the arterial pulsation especially in obese patients. Get an assistant to retract the abdomen if this is a problem and recheck the landmarks.
Complications
Early: haematoma; arrhythmia; accidental arterial puncture; pneumothorax; haemothorax; air embolism
Late: infection; thrombosis; vascular erosion
Catheter tip position
The CVC tip should lie in the superior vena cava at the level of the carina on chest x-ray. If the CVC is within the right atrium it is in too far and should be withdrawn. Ideally the tip of the CVC should not abut the side of the vessel wall as this can lead to erosion of the vein wall.
Spinal and epidural anaesthesia
Anatomy (see Figure 29.1)
The spinal cord terminates at L1–2 in the adult, L3 in children.
Below this level the lumbar and sacral nerves form the cauda equina.
The meninges (dura, arachnoid and pia mater) surround the spinal cord from the foramen magnum to S2 level.
Dural cuffs extend laterally as far as intervertebral foraminae.
There is a potential space between the dura and arachnoid mater – the subdural space; inadvertent injection into this space is a recognized complication of spinal and epidural injections.
The epidural (extradural) space lies between the walls of the spinal canal and the spinal dural mater. It is a potential, low pressure space filled with fat, areolar tissue and the internal vertebral venous plexus.
The ligamentum flavum links the vertebral laminae and is at its thickest in the lumbar region.
Spinal
Indications
Wide variety of elective and emergency surgery below the level of the umbilicus (T10).
Approaches and landmarks
Sitting or lateral position with spine flexed.
Line between iliac crests (Tuffier’s line) passes across L4 and is used to locate L3–4 space, which is most commonly used.
Midline and paramedian approaches can be used.
Paramedian – 1–2 cm lateral to upper border of spinous process, insert needle perpendicular to skin and advance to contact bone (lamina), then withdraw and re-angle 15 degrees medially and 30 degrees cephalad to pass over lamina and enter interlaminar space.
Insertion
Sterilize skin using 0.5% chlorhexidine spray and allow it to dry.
Drape and use 1% lidocaine to skin if patient awake.
Insert introducer needle at 90 degrees to skin in midline.
Spinal needle passes through introducer into supraspinous and interspinous ligaments then the tougher ligamentum flavum and through the dura (see Figure 29.1).
If bone is contacted withdraw and redirect needle, cephalad in first instance.
Following dural puncture cerebrospinal fluid (CSF) should flow freely.
Bupivacaine 0.5% heavy or plain. Plain produces a less reliable block and approximately 0.5 ml more volume is required for a similar level block.
Ropivacaine not licenced for intrathecal use.
Opioids commonly added are diamorphine 0.25–0.5 mg or fentanyl 10–25 mcg.
Tips and advice
Position of patient and comfort of operator are key to success, do not be tempted to rush or compromise.
Accurate identification of L3/4 space is difficult, 70% of clinicians are higher than they think.
If a second space is attempted go down as level of termination of the conus is variable.
Sitting position allows easier identification of the midline and gives higher CSF pressure so improves flow.
Lateral position allows possibility of sedation.
Anatomy of the subarachnoid and epidural space.
Epidural
Indications
Anaesthesia in abdominal and lower limb surgery.
Acute pain relief post-operatively in thoracic, abdominal or lower limb surgery, labour, trauma and for miscellaneous reasons (e.g. pancreatitis, ischaemic pain).
Chronic pain states.
Approaches and landmarks
Position as for spinal.
Identify the appropriate vertebral space (use landmarks of Tuffier’s line indicating spinous process of L4 or tip of scapula is level with T7 and count spaces to correct level).
Midline/paramedian approaches can be used (as for spinal).
Insertion
Prepare trolley (see Figure 29.2) and flush the catheter and filter with saline to ensure free passage.
Clean, drape and infiltrate 1% lidocaine as for spinal. You can use slightly more lidocaine and use the injecting needle to seek the space and infiltrate local into the interspinous ligaments.
Insert the Tuohy needle in the direction indicated, the higher the level the more cephalad the angle is likely to be. When resistance becomes more obvious remove the trocar.
Attach the loss of resistance syringe filled with saline (or air) and carefully advance into ligamentum flavum, constantly checking for loss of resistance as the needle is advanced through the ligament.
On loss of resistance immobilize the Tuohy and check no blood or CSF flows from the Tuohy needle.
Note the depth and insert the catheter generously.
Remove the Tuohy over the catheter and pull back to leave 4–5 cm in the space.
Check for absence of blood or CSF and look for a meniscal drop.
Fix the catheter to the skin with a sterile see-through dressing to allow site inspection.
Fix catheter well up back and over shoulder.
Drugs
Opioids commonly added are diamorphine 2.5–5 mg or fentanyl 50–100 mcg.
Tips and advice
Many factors affect spread of epidural solutions; therefore, an understanding of these allow manipulation of the block.
Drug mass is critical and more important than volume, for a given mass a larger volume will spread more.
Epidural space increases in volume in a caudal direction so larger volumes are required to achieve the same dermatomal cover the lower the epidural is sited.
Smaller volumes may be needed in age >40, pregnancy and morbid obesity.
Position can be used to manipulate the block, sitting will reduce upward spread.
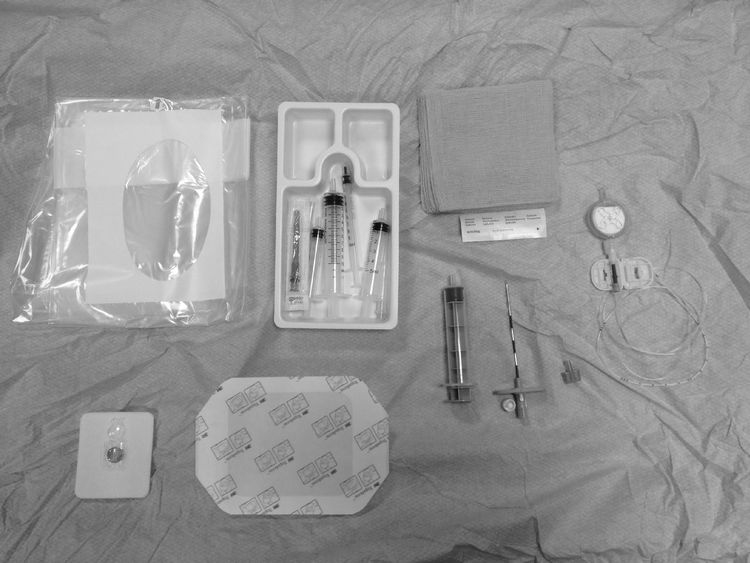
Epidural trolley.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


