TABLE 12.1.General, Supportive, and Emergency Measures in Drug Overdose or Poisoning*
For poisoning emergency call 1-800-222-1222. The call is routed to the local poison control center serving the caller based on area code and exchange of the caller. The number is functional 24 hours/day in all 50 states, the District of Columbia, the U.S. Virgin Islands, and Puerto Rico.
May cause seizures with cocaine May increase risk of ventricular tachycardia with antidepressant overdose
Tachyarrhythmias: β-blockade
May lead to unopposed α-adrenergic effects and coronary vasoconstriction in cocaine overdose May increase risk of ventricular tachycardia in cyclic antidepressant overdose Wide QRS tachycardia (if tricyclic antidepressant suspected or cocaine overdose): NaHCO3 50–100 mEq IV
Coma
Airway, ventilation, oxygenation, IV access Dextrose 50%, 50–100 mL IV Thiamine 100 mg IV (especially if history of alcoholism)
Naloxone (IV/IM, or via endotracheal tube) 0.2–0.4 mg IV; in patients with suspected narcotic addiction 2 mg q 2–3 min until 10 mg total given
May precipitate withdrawal Synthetic opioids, such as fentanyl, may require larger doses
Flumazenil 0.2 mg q 30–60 sec, total dose 3–5 mg IV if sedative-hypnotic overdose suspected
Contraindicated in patients with epilepsy receiving long-term benzodiazepine therapy and in severe mixed overdose with benzodiazepine and a proconvulsant drug (i.e., aminophylline, amitriptyline, or chloroquine)
Gastrointestinal decontamination
(See specific poisoning for indications)
Ipecac syrup: 30 mL followed by 8 oz water, may repeat after 30 min; nausea and vomiting may delay the use of activated charcoal for up to 6 h
Contraindicated if drowsy, unconscious, convulsing, hydrocarbon ingestion, corrosive poisoning, or rapidly acting convulsants (strychnine, camphor, tricyclic antidepressants)
Gastric lavage: stomach tube; 37–40F, usually most effective within first 4 h after overdose; lavage with 100–200 ml aliquots of 0.9% NaCl or water, usually 1–2 L sufficient to clear contents
Contraindicated in stuporous or comatose patient with absent gag unless intubated with endotracheal tube
Activated charcoal: 1–2 g/kg oral aqueous slurry with sorbitol cathartic with first dose and then q 2nd or 3rd dose; repeat dose 20–30 g q2–4h; may hasten drug elimination but cathartics should not be used with each dose
Contraindicated in stuporous, omatose, or convulsing patient unless airway protected by endotracheal tube and gastric tube in place
Catharsis: Magnesium sulfate 10%, 2–3 mL/kg PO or sorbitol 70%, 1–2 mL/kg PO
Contraindications: magnesium-based cathartics may accumulate in renal failure, oil-based cathartics carry risk of aspiration, sodium-based cathartics may exacerbate hypertension or heart failure
Whole bowel irrigation: polyethylene glycol, electrolyte solution (COLYTE, GoLYTELY) 1–2 L/h via gastric tube until rectal effluent clear to push tablets through GI tract (especially iron ingestion, sustained release and enteric coated tablets)
Pharmacobezoars may form from sustained-release products and result in continual drug absorption after gastrointestinal decontamination
May require endoscopic identification and removal or surgical removal if intestinal obstruction
Nitroprusside 0.25–10 μg/kg/min or Phentolamine 2–5 mg IV; add β-blocker as needed
β-blockade may lead to unopposed α-adrenergic effects and coronary vasoconstriction in cocaine overdose
Hyperthermia (>40°C)
Rapid cooling measures and benzodiazepines to decrease heat production if agitated or seizing
If ineffective and extreme muscle rigidity present, then neuromuscular blockade (see Tables 2.4 and 2.5)
If malignant hyperthermia, dantrolene 2.5 mg/kg IV (see Table 2.14)
If neuroleptic malignant syndrome, bromocriptine 2.5–7.5 mg PO qd or dantrolene 2.5 mg/kg IV (maximum total dose 10 mg/kg)
Hypotension
Fluid resuscitation
Vasopressor (e.g., dopamine)
If suspected/documented overdose is:
tricyclic antidepressant: NaHCO3 IV 1–2 mEq/kg
β-blocker: glucagon 5–10 mg IV
calcium antagonist: calcium chloride 10% 10–15 ml IV
Renal excretion
Forced diuresis and urinary pH manipulation: limited utility of alkaline diuresis, 50–100 mEq of NaHCO3 in 1 L of 0.2% NaCl or D5W to urinary pH of 7–8 to prevent tubular reabsorption of acidic drugs, such as phenobarbital, salicylates, and isoniazid
Monitor for hypokalemia, metabolic alkalosis, hypernatremia
Dialysis indicated if lethal amounts of dialyzable drug present
Diazepam 2.5–10 mg IV Lorazepam 2–3 mg IV Midazolam 5–10 mg IV or IM Phenobarbital 10–20 mg/kg IV (over 30 min)
Phenytoin 10–20 mg/kg (infusion should not exceed 50 mg/min)
GI, gastrointestinal; IM, intramuscular; IV, intravenous; PO, by mouth
*Fifty percent of all adult overdoses and 90% of all opioid overdoses are mixed ingestions. Most frequently abused: alcohol in combination with drugs, cocaine, heroin or morphine, acetaminophen, aspirin, marijuana, alprazolam, ibuprofen, diazepam, amitriptyline.
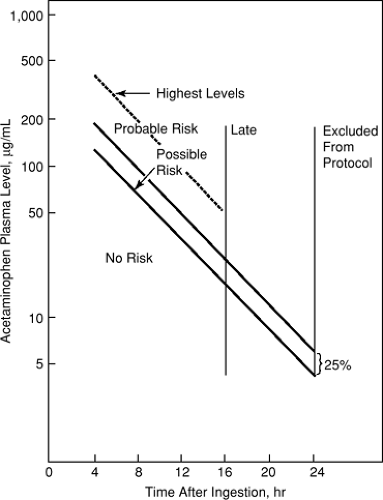
FIGURE 12.1. Acetaminophen Overdose: N-acetylcysteine Dosing Nomogram Acetaminophen treatment protocol. (Adapted from Rumack BH, Peterson RC, Koch GG, et al. Acetaminophen overdose. 662 cases with evaluation or oral acetylcysteine treatment. Arch Intern Med 1981;141:382. Used with permission.)
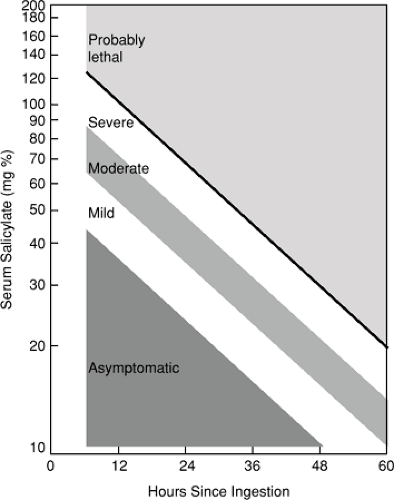
FIGURE 12.2. Salicylate Overdose Nomogram Nomogram relating serum salicylate level to severity of intoxication.
Mild toxicity: mild to moderate hyperpnea without acidosis, lethargy, and vomiting.
Moderate toxicity: severe hyperpnea with acidosis, marked lethargy or excitability but no coma or convulsions, and marked gastrointestinal distress.
Severe toxicity: severe hyperpnea, severe neurologic impairment that may include coma or convulsions and marked acidosis.
(Adapted from
Done AK. Aspirin overdose: incidence, diagnosis and management. Pediatrics 1978;62(suppl):895.
Reproduced with permission.)
TABLE 12.2. Specific Therapy for Poisonings and Overdoses
Agent Ingested
Emergency/Supportive Care
Specific Therapy
Comments
Acetaminophen
Empty stomach (emesis or lavage) Activated charcoal
Acetylcysteine Oral solution; load 140 mg/kg then 70 mg/kg q4h × 17 doses IV solution; load 150 mg/kg IV over 15 min, then 50 mg/kg infuse over 4 h, then 100 mg/kg infuse over 16 h
Refer to nomogram (Figure 12.1) to predict risk of toxicity Serum acetaminophen levels should be obtained (see Table 12.4). Levels 0–4 h after ingestion uninterpretable; NAC administration has priority over charcoal if levels are toxic Best if given within 8–10 h of overdose Narcotics and anticholinergics may interfere with oral absorption IV formulation may cause anaphylactoid reaction; interrupt infusion until allergic symptoms treated
Acid corrosives (pool, toilet bowl cleaners)
Do not induce emesis Dilute by drinking 8 oz milk or water Do not give bicarbonate Immediate lavage if possible
Surgical intervention for perforation, peritonitis, bleeding
UGI endoscopy to assess extent of tissue damage, do not pass beyond site of injury
Alkalis (lye, oven cleaners, Clinitest tablets, drain cleaners, disk batteries)
Do not induce emesis Dilute by drinking milk or water Immediate lavage if possible
Endoscopic removal of batteries Surgical intervention for perforation, peritonitis, bleeding
UGI endoscopy to assess extent of tissue damage, do not pass beyond site of injury
Airway, assisted ventilation Do not induce emesis (seizure risk) Gastric lavage Activated charcoal
Agitation or psychosis; diazepam 5–10 mg IV or midazolam 0.1–0.2 mg/kg IV/IM, lorazepam 1–2 mg IV Hypertension: labetalol 10–20 mg IV, or phentolamine 1–5 mg IV, or nifedipine 10–20 mg PO Tachyarrhythmias: esmolol 50–300 μg/kg/min IV
β-adrenergic blocker alone can worsen hypertension due to unopposed α adrenergic effects
Antiarrhythmics (class IA: quinidine, procainamide, disopyramide; class IC: flecainide)
Activated charcoal and cathartic
Atrioventricular block, hypotension, QRS interval widening: sodium bicarbonate 50–100 mEq IV Torsade de pointes: magnesium sulfate 1–2 g IV or isoproterenol 1–5 μg/min or overdrive pacing
Anticoagulants (warfarin, rodenticides)
Emesis or gastric lavage Activated charcoal
If prothrombin time elevated, give phytonadione (vitamin K) 5–10 mg IV If serious bleeding, give fresh frozen plasma to correct coagulopathy Recombinant activated factor VII (off label use) 15–30 μg/kg IV q12h life threatening bleeding may use 90–120 μg/kg IV bolus q2h
Antidepressants (tricyclic or tetracyclic, amitriptyline, maprotiline)
Airway, assisted ventilation Do not induce emesis (seizure risk) Gastric lavage Activated charcoal
Cardiotoxic effects: (supraventricular and ventricular tachycardias) sodium bicarbonate 50–100 mEq IV and specific therapy, alkalinize blood pH to 7.5 Seizures: diazepam 5–10 mg IV q1–2h prn Hyperthermia: sedate and paralyze Hypotension: volume resuscitation and then dopamine 5–20 μg/kg/min or norepinephrine 5–100 μg/min or epinephrine 1–20 μg/min
QRS widening >0.10 correlates with increased risk of seizure, >0.16 increased risk of seizure and arrhythmias Class 1A (quinidine, disopyramide, procainamide), and class 1C (e.g., flecainide) contraindicated Phenytoin may worsen risk of ventricular tachycardia β-blockade may worsen cardiac depression and hypotension Physostigmine, a cholinergic agonist, may cause seizures, ventricular fibrillation, and asystole Flumazenil contraindicated; may aggravate seizures and cardiotoxicity
Airway, assisted ventilation Emesis or gastric lavage Activated charcoal Cathartic
Supportive therapy with fluids and vasopressor support (e.g., dopamine, Table 3.8)
Arsenic
Emesis or gastric lavage Activated charcoal Supportive care with IV fluids
Antidote for massive overdose; dimercaprol injection (BAL), 10% solution in oil, 2–3 mg/kg IM q4h × 48 h, q6h × 24, then q12h for 10 d, pretreat with diphenhydramine 25–50 mg PO Follow with dimercaptosuccinic acid (succimer) 10 mg/kg/dose PO q8h × 5d, then q12h × 14d
Atropine (anticholinergics)
No emesis if antidepressants with anticholinergic effects ingested, due to seizure risk, otherwise: Emesis or gastric lavage Activated charcoal
If pure atropine overdose, administer physostigmine salicylate 0.5–1 mg IV over 5 min, with ECG monitoring
Sedation and cooling measures (tepid baths, cooling blanket for increased temperature)
β-adrenergic blockers
Airway, assisted ventilation Do not induce emesis (seizure risk) Empty stomach by gastric lavage Activated charcoal
Bradycardia or AVB: atropine 0.5–2 mg IV, isoproterenol 2–20 μg/min IV, or pacemaker (transvenous or transcutaneous) If above fail, glucagon 5 mg IV followed by infusion 1–5 mg/h
Catecholamine infusion alone may lead to arrhythmias or hypotension. Use in conjunction with IV calcium chloride 1 gm of a 10% solution (10mL) via central line slow infusion, max 3 g and/or insulin 0.1 units/kg/h with glucose 1 gm/kg/h (continued next page) Monitor glucose levels q30–60 min for first 4 h
Benzodiazepines
See Sedative-hypnotics
Calcium channel blockers
Airway, assisted ventilation Do not induce emesis (seizure risk) Gastric lavage Activated charcoal
Bradycardia, AV block: atropine 0.5–2 mg IV, isoproterenol 2–20 μg/min IV, or pacemaker (transvenous or transcutaneous) Negative inotropic effects: calcium chloride 10% 5–10 ml IV or calcium gluconate 10% 10–15 ml IV Epinephrine infusion 1–4 μg/min Glucagon 5 mg IV followed by infusion 1–5 mg/h Insulin 0.1 unit/kg/h with glucose 1 gm/kg/h Monitor glucose levels q30–60 min for first 4 h
Carbon monoxide (CO)
Airway, assisted ventilation
100% O2 via tight fitting mask or endotracheal tube Hyperbaric O2 may be useful for patients with coma, seizure, pregnancy
Half life of CO is 4–5 h breathing room air but is reduced by high FiO2
Do not induce emesis (seizure risk) Gastric lavage Activated charcoal
Diazepam 5–10 mg IV for seizures
Cocaine
Airway, supplemental oxygen
Anxiety, agitation, seizures: IV diazepam, or lorazepam Hyperthermia: rapid cooling, benzodiazepine Hypertension: benzodiazepine IV, nitroprusside or phentolamine Arrhythmias (QRS prolongation): NaHCO3 1–2 mEq/kg IV Myocardial ischemia: aspirin, nitroglycerin or calcium-channel blocker (see Table 3.1)
Excess sympathetic tone (centrally mediated) contributes to agitation, seizures, hypertension, tachyarrhythmias and is treated with benzodiazepines β-blockade may lead to unopposed α-adrenergic effects and worsen coronary vasoconstriction Associated with rhabdomyolysis
Cyanide
Airway and assisted ventilation For ingestion: emesis or gastric lavage and activated charcoal
Cyanide antidotes: (a) amyl nitrate inhalant 0.3 ml q3min × 2 (b) sodium nitrite 6 mg/kg IV over 3–5 min (c) sodium thiosulfate 250 mg/kg IV (usually 50 ml or 12.5 g of a 25% solution) Decrease or discontinue nitroprusside infusion
Elevated venous oxygen saturation (>90%) Nitrites induce methemoglobinemia which binds free cyanide (may induce hypotension); thiosulfate promotes conversion of cyanide to thiocyanate (see Table 12.4)
Digitalis, cardiac glycosides
Airway and assisted ventilation Do not induce emesis (enhanced vagotonia) Gastric lavage Activated charcoal
Monitor potassium Ventricular arrhythmias: lidocaine (1–3 mg/kg IV) or phenytoin (10–15 mg/kg IV over 30 min) Bradycardia (atropine 0.5–2 mg IV), isoproterenol 2–20 μg/min or pacemaker transvenous or transcutaneous)
Identify and correct hypovolemia, hypoglycemia, respiratory monitoring and IV thiamine (100 mg) in patients at risk for Wernicke’s encephalopathy Severe metabolic acidosis with increased anion gap may indicate cointoxication with other alcohols (methanol, ethylene glycol) Increased levels of ketones or acetones may indicate isopropyl alcohol ingestion
Ethylene glycol or methanol
Airway and assisted ventilation Emesis or gastric lavage Activated charcoal (limited effectiveness)
Fomepizole as soon as possible; loading dose 15 mg/kg IV in 100 mL D5W over 30 min, followed by 10 mg/kg IV q12h or 48 h, then 15 mg/kg q12h until ethylene glycol levels reduced (<20 mg/dL) or methanol levels reduced (<50 mg/dL), pH is normal, and patient is asymptomatic Dialysis should be considered in addition to fomepizole if renal failure present, worsening acidosis, or if elevated levels (>20 mg/dL ethylene glycol or >50 mg/dL methanol) Metabolic acidosis: sodium bicarbonate 50–100 mEg IV Ethanol: (alternative therapy if fomepizole unavailable) loading dose 750 mg/kg PO or IV (as 5% to 10% solution), maintenance 100–150 mg/kg/h (increase to 175–250 mg/kg/h during hemodialysis)
Fomepizole rapidly competitively inhibits alcohol dehydrogenase. It prolongs half-life of ethanol and simultaneous use not recommended Fomepizole is dialyzable and dose frequency should be increased to q4h during dialysis Adjunctive therapy for ethylene glycol poisoning; pyridoxine 50 mg IV/IM q6h and thiamine 100 mg IV/IM q6h and consideration of forced diuresis with fluids and mannitol to prevent oxalate crystal injury to renal tubules Methanol poisoning; folate 50–70 mg IV q4h × 24 h Maintain serum ethanol concentration 100–130 mg/dl (See Table 12.4)
Hallucinogens
(LSD, mescaline, 3, 4 methylene- dioxymethamphetamine; “ecstasy” or MDMA, methylenedioxy-amphetamine or MDA
Only gold members can continue reading. Log In or Register to continue