CHAPTER 126
“Plantaris Tendon” Rupture, Gastrocnemius Muscle Tear
(Calf Muscle Tear)
Presentation
The patient will come in limping, having suffered a whiplike sting in the calf while stepping off the foot hard or attempting a lunging shot during a game of tennis or similar activity. The patient may have actually heard or felt a “snap,” described as being like the “pop” of a champagne cork, at the time of injury or may think someone actually kicked or shot him in the calf. The deep calf pain persists and may be accompanied by mild to moderate swelling and ecchymosis. Neurovascular function will be intact.
What To Do:
 Obtain a clear history of the mechanism of injury, either forceful ankle plantar flexion or knee extension while the foot is dorsiflexed, as is seen on the back leg during the “push off” of a lunging tennis shot. Pain may radiate to the knee or ankle.
Obtain a clear history of the mechanism of injury, either forceful ankle plantar flexion or knee extension while the foot is dorsiflexed, as is seen on the back leg during the “push off” of a lunging tennis shot. Pain may radiate to the knee or ankle.
 Perform a physical examination, which should reveal calf tenderness, especially along the medial musculotendinous junction of the medial gastrocnemius. There may be a defect in the muscle belly itself. Swelling will usually be asymmetric, and over time, any ecchymosis may be found spreading to a more dependent site over the ankle or foot. Dorsiflexion of the foot and resisted plantarflexion are typically painful. Peripheral pulses should be present and symmetric.
Perform a physical examination, which should reveal calf tenderness, especially along the medial musculotendinous junction of the medial gastrocnemius. There may be a defect in the muscle belly itself. Swelling will usually be asymmetric, and over time, any ecchymosis may be found spreading to a more dependent site over the ankle or foot. Dorsiflexion of the foot and resisted plantarflexion are typically painful. Peripheral pulses should be present and symmetric.

 Rule out an Achilles tendon rupture, because this needs orthopedic evaluation for possible surgery. Palpate the Achilles tendon for a defect or deformity, which represents a torn segment. Squeeze the gastrocnemius muscle just distal to its widest girth, with the patient kneeling on a chair or lying prone on a stretcher with the legs overhanging the end (Figure 126-1) to examine for normal plantar flexion of the foot. Alternatively, the test may be performed with the patient’s knees flexed and the feet up while he is supine. Always compare the affected leg with the contralateral limb. The resultant plantar flexion will be totally absent with a complete Achilles tendon tear. A defect in the contour along the length of the Achilles tendon, pain distal to the body of the gastrocnemius, and lack of pain with palpation of the muscle belly are all typical of Achilles tendon rupture and not plantaris tendon rupture or a gastrocnemius tear.
Rule out an Achilles tendon rupture, because this needs orthopedic evaluation for possible surgery. Palpate the Achilles tendon for a defect or deformity, which represents a torn segment. Squeeze the gastrocnemius muscle just distal to its widest girth, with the patient kneeling on a chair or lying prone on a stretcher with the legs overhanging the end (Figure 126-1) to examine for normal plantar flexion of the foot. Alternatively, the test may be performed with the patient’s knees flexed and the feet up while he is supine. Always compare the affected leg with the contralateral limb. The resultant plantar flexion will be totally absent with a complete Achilles tendon tear. A defect in the contour along the length of the Achilles tendon, pain distal to the body of the gastrocnemius, and lack of pain with palpation of the muscle belly are all typical of Achilles tendon rupture and not plantaris tendon rupture or a gastrocnemius tear.
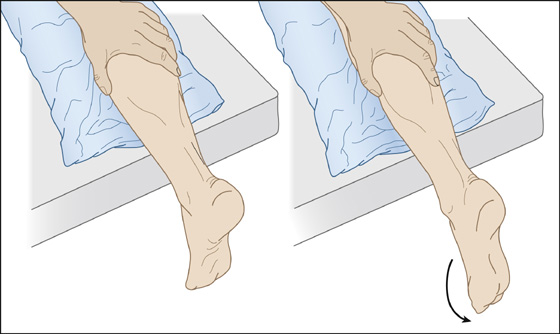
Figure 126-1 Thompson, Simmonds, or “calf squeeze” test.
 When there is any uncertainty, a definitive diagnosis can be established with ultrasonography or MRI. With any Achilles tendon tear, orthopedic consultation is necessary.
When there is any uncertainty, a definitive diagnosis can be established with ultrasonography or MRI. With any Achilles tendon tear, orthopedic consultation is necessary.
 If there is excruciating pain out of proportion to what would be expected with these injuries, the possibility of an acute compartment syndrome must be entertained, and immediate orthopedic consultation should be obtained.
If there is excruciating pain out of proportion to what would be expected with these injuries, the possibility of an acute compartment syndrome must be entertained, and immediate orthopedic consultation should be obtained.
 When serious conditions have been ruled out, provide the patient with elastic support (e.g., Ace bandage, antiembolism stocking, Tubigrip) from the foot to the tibial tuberosity, with or without a posterior splint to provide additional comfort. Gravity equinus (allowing the toe to drop down naturally) is generally the most comfortable position.
When serious conditions have been ruled out, provide the patient with elastic support (e.g., Ace bandage, antiembolism stocking, Tubigrip) from the foot to the tibial tuberosity, with or without a posterior splint to provide additional comfort. Gravity equinus (allowing the toe to drop down naturally) is generally the most comfortable position.
 Patients with severe pain may require crutches for several days. Some clinicians have begun using rocker-bottom postoperative boots for early ambulation.
Patients with severe pain may require crutches for several days. Some clinicians have begun using rocker-bottom postoperative boots for early ambulation.
 Have the patient keep the leg elevated above the level of his heart and at rest as much as possible for the next 24 to 48 hours, initially applying cold packs intermittently.
Have the patient keep the leg elevated above the level of his heart and at rest as much as possible for the next 24 to 48 hours, initially applying cold packs intermittently.
 An analgesic such as hydrocodone (e.g., Lorcet, Lortab) may be helpful initially, as well as nonsteroidal anti-inflammatory drugs (NSAIDs), if tolerated.
An analgesic such as hydrocodone (e.g., Lorcet, Lortab) may be helpful initially, as well as nonsteroidal anti-inflammatory drugs (NSAIDs), if tolerated.
 The temporary use of bilateral 1-inch heel wedges may also provide immediate comfort for ambulatory patients. Encourage patients to return to a heel-toe walking sequence as quickly as possible. When this is achieved, they can discontinue using the heel lift.
The temporary use of bilateral 1-inch heel wedges may also provide immediate comfort for ambulatory patients. Encourage patients to return to a heel-toe walking sequence as quickly as possible. When this is achieved, they can discontinue using the heel lift.
 Gentle stretching may be initiated as soon as it can be accomplished without pain. Strengthening may begin as soon as 24 hours after the initial injury. Massage is helpful as an adjunct to a strengthening program.
Gentle stretching may be initiated as soon as it can be accomplished without pain. Strengthening may begin as soon as 24 hours after the initial injury. Massage is helpful as an adjunct to a strengthening program.
 Patients should be reassured about the generally benign nature of this injury and the excellent chance for a full recovery. They should also be warned about potentially alarming ecchymosis that may develop in the days following the injury and reassured that this is a benign phenomenon.
Patients should be reassured about the generally benign nature of this injury and the excellent chance for a full recovery. They should also be warned about potentially alarming ecchymosis that may develop in the days following the injury and reassured that this is a benign phenomenon.
 Athletes generally can return to training and competition in 4 to 6 weeks following the injury, although severe tears may take up to 12 weeks to heal. Sports-specific activities can be resumed once the athlete is pain free with full and symmetric range of motion (ROM) and full strength has been regained. Strengthening and stretching should continue for several months to overcome the increased risk for reinjury resulting from the deposition of scar tissue involved in the healing process.
Athletes generally can return to training and competition in 4 to 6 weeks following the injury, although severe tears may take up to 12 weeks to heal. Sports-specific activities can be resumed once the athlete is pain free with full and symmetric range of motion (ROM) and full strength has been regained. Strengthening and stretching should continue for several months to overcome the increased risk for reinjury resulting from the deposition of scar tissue involved in the healing process.
What Not To Do:
 Do not bother getting radiographs of the area unless there is a suspected associated bony injury. This is a soft tissue injury that is not generally associated with fractures.
Do not bother getting radiographs of the area unless there is a suspected associated bony injury. This is a soft tissue injury that is not generally associated with fractures.
 Do not attempt to evaluate Achilles tendon function merely by asking the patient to plantarflex the foot. Achilles tendon function is only isolated with the calf squeeze test.
Do not attempt to evaluate Achilles tendon function merely by asking the patient to plantarflex the foot. Achilles tendon function is only isolated with the calf squeeze test.
Discussion
The main function of the gastrocnemius muscle is to plantarflex the ankle. The plantaris muscle is a pencil-sized structure tapering down to a fine tendon that runs beneath the gastrocnemius and soleus muscles to attach to the Achilles tendon or to the medial side of the tubercle of the calcaneus. The function of the muscle is of little importance, and, with rupture of either the muscle or the tendon, the transient disability is due only to the pain of the torn fibers or swelling from the hemorrhage. Most instances of “tennis leg” are now thought to be the result of partial tears of the medial belly of the gastrocnemius muscle or to ruptures of blood vessels within that muscle. Throughout the belly of the muscle, the medial gastrocnemius has several origins of tendinous formation. Most strains or tears occur at this musculotendinous junction. The greater the initial pain and swelling, the longer one can expect the disability to last.
Tendon ruptures typically affect men in their third or fourth decade who are active in sports. The average occurrence of a gastrocnemius muscle tear is in the fourth to sixth decade. A tendon rupture is usually an indicator of intratendinous degenerative changes.
Achilles tendon injury can occur with the identical mechanism of a plantaris tendon or medial gastrocnemius rupture. Because the pain and debility may be similar, clinical differentiation is sometimes difficult.
The diagnosis of Achilles tendon rupture is missed by the initial examiner in up to 25% of patients. One misleading finding is that the patient is able to plantarflex the foot with no resistance, because several other muscles (toe flexors, peroneus) also perform this action. The expected defect in the tendon may also be obscured by edema or hemorrhage. The squeeze test (Thompson or Simmonds test) is usually an infallible sign of complete rupture, but a false negative might arise if the plantaris tendon is left intact. Imaging techniques—including real-time high-resolution ultrasonography and MRI—are now used to aid diagnosis. Ultrasonography usually costs less than MRI; however, when “limited MRI protocols” are available and only a few images of the suspected region of disease are obtained, pricing can be competitive and will give images superior to ultrasonography.
Other entities that can be confused with plantaris tendon and medial gastrocnemius rupture are Baker cyst rupture and deep venous thrombosis. When physical findings are dubious, the history along with Doppler ultrasonography will often help clarify the diagnosis.
Direct injection of steroids and administration of systemic corticosteroids and fluoroquinolone antibiotics are associated with an increase in the risk for Achilles tendon rupture. Other disease processes, such as rheumatoid arthritis, systemic lupus erythematosus, chronic renal failure, hyperuricemia, genetically determined collagen abnormalities, arteriosclerosis, and diabetes mellitus, have been implicated as risk factors for rupture. With age, tendons stiffen from the effects of reduced glycosaminoglycan content and increased collagen concentration. Blood and nutrient supply also are reduced with age.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


