Method
IP or OP treatment
Dressing changes required
Weeks to healing (average)
Recurrence (%)
Abscess drainage/Shaving
OP
Yes
3–4
25–40
Excision
OP
No
3
16
Fistulotomy
OP
Yes
4–6
1–19
Marsupialization
OP
Yes
6
8
Wide local excision only
OP
Yes
8
Up to 38
Wide local excision, primary closure
OP
No
4–8
Up to 38
Excision, advancement flap
IP
No
3–4
6–20
Karydakis advancement flap
IP
No
3
1.3
Cleft closure
OP
No
3
3.3
Perioperative Care
Preoperative Preparation
Acute infection should be resolved prior to definitive operation. Abscesses should be drained and cellulitis treated with antibiotics. Most patients are under the age of 40; therefore, minimal preoperative testing is required. Smoking cessation should be encouraged to assist wound healing.
Positioning and Anesthesia
After general anesthesia is induced, the patient is placed in the prone jack-knife position. Tape to spread the gluteus facilitates full visualization of the cleft. Hair is clipped in the affected area. Patients are administered intravenous antibiotics prior to surgical incision.
Description of Procedures
Many operations have been described for the treatment of pilonidal disease. Few have been studied in a randomized controlled fashion. Therefore, recommendations on operative approach are difficult to make. However, we prefer to start with the simplest operation and advance our interventions to the more complex as necessary. Below we describe the operative approaches employed at our institution.
Incision and Curettage
Sinus tracts are identified with a probe and opened longitudinally using a knife or bovie cautery. The wound base is then curetted, and the skin edges are excised in order to expose the open granulating wound. The wound heals by secondary intention, and must be kept clean and free of hair. The patients are then advised to partake in BID postoperative wound care to allow for adequate healing. Alternatively, a wound vacuum can be employed to assist in wound care and shorten the length of healing.
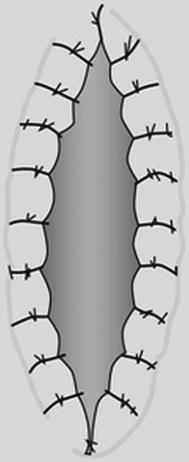
Marsupialization
If a sinus is infected at the time of excision, primary closure should be avoided. Marsupialization is a technique by which the surrounding skin edges of a defect are sutured down to the presacral fascia [1]. Sinus tracts are identified and typically excised but can be unroofed. The wound base is curetted and all hair is removed. The defect that remains is often large and requires significant dressing changes. Therefore, the skin edges are sewn to the fibrotic wound base or presacral fascia using interrupted 3-0 vicryl suture (Fig. 27.1). This decreases the size of the wound significantly and anecdotally shortens healing time. Figures 27.2, 27.3, 27.4, 27.5, and 27.6 demonstrate this operative technique in a patient with recurrent pilonidal disease.