Fig. 7.1
The bevel of the needle should be cephalad (b) and the lead should be introduced with the goal of placement within the posterior epidural space (a)
Once the needle has been addressed, the next component to examine should be the lead itself. Issues to consider are the type of stylet (Fig. 7.2a), length of lead, and whether the position is ideal for initial exit from the needle to start on a correct path toward the target. Initially in most cases the curved stylet is the initial starting point for lead placement. In situations in which the lead is advancing too far laterally, a change to a straight stylet (Fig. 7.2b) may allow the lead to correct toward the midline. In some clinical settings the physician may need to alternate between a curved and a straight stylet several times to maneuver the lead to the desired location. The need to exaggerate the curve in the stylet is rare, but in some cases the physician may create an exaggerated curve creating a “hockey stick” angle that is needed to drive the lead toward midline when it is tracking laterally. In cases in which an exaggerated stylet is used, the physician should reconfirm placement of the lead with both fluoroscopy and computer screening once the stylet is removed to detect a “rebound movement” that results in lead movement once the rigidity of the stylet is removed. Lead issues are reviewed in Table 7.1. New stylets with polymer coatings may allow for easy lead placements and stylet removal without lead contour changes. Despite this advance the lead can still be difficult to place.
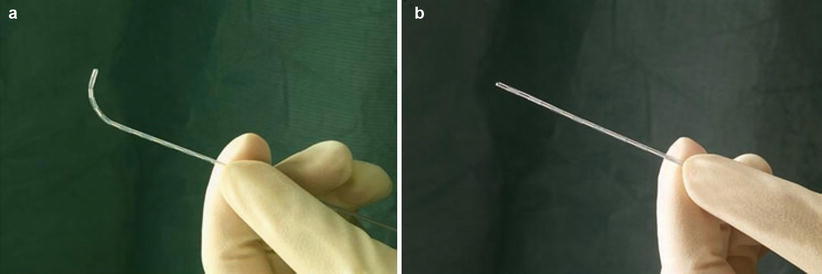
Fig. 7.2
(a) Curved stylet; (b) Straight stylet
Table 7.1
Lead issues
Lead issue | Options |
|---|---|
Lateral lead movement | Rotate the lead using a curved stylet |
Obstruction to movement | Gently reposition the lead alternating the curved and straight stylets |
Gently tap the lead against the obstruction on multiple rapid attempts, withdrawing slightly each time | |
Use the wire coil to pass the obstruction (use caution and stop if pain occurs) | |
Failure to achieve stimulation despite optimal X-ray placement | Troll with the lead to find an area responsive to stimulation, try different programming arrays including a guarded cathode |
High impedance of the lead | Reposition the lead cephalad or caudad |
Epidural obstructions can be frustrating and potentially dangerous when attempting to successfully place a lead. These obstructions can be caused by several factors (Table 7.2) and can lead to a failure of the procedure. All manufacturers include a wire coil in their typical lead deployment kit. This coil wire can be used to create a pathway or channel in the epidural space to help with lead advancement. These wire inserts can be helpful, but they can also lead to complications and should be used with caution. The authors prefer a different method for overcoming this issue. That is to use a technique of finesse and a gentle approach to avoid trauma. In this method the lead is advanced to the point of obstruction and then repeatedly advanced forward. Each time an obstruction is felt, the lead is withdrawn, and then advanced only during exhalation. In many cases this method will lead to an ability to advance the lead without traumatizing the tissue. Other options include using the curved and straight stylet to “drive” around the obstructive structure. In the event that these methods are unsuccessful, a different intralaminar level of entry should be considered. If difficulty persists past a reasonable number of attempts, the procedure should be aborted and a surgical laminotomy approach should be considered, even for the trial phase.
Table 7.2




Causes of obstructions
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
