KEY POINTS
Fever occurs in more than 50% of patients at some time during their ICU stay.
Approximately 50% of fevers are due to noninfectious causes, such as drug fevers, surgical trauma, and central nervous system injury.
A thoughtful evaluation of a fever may reduce costs and lessen the potential risk to the patient.
Extreme elevations of temperature (>41.1°C) are most often not due to infectious etiologies.
Heat stroke, serotonin syndrome, neuroleptic malignant syndrome, and malignant hyperthermia are life-threatening causes of hyperpyrexia that must be immediately recognized and treated in order to avoid multisystem organ failure and death.
Although fever is associated with adverse outcomes in the ICU, there is no conclusive evidence to support the routine treatment of fever due to infection in non-brain-injured patients.
INTRODUCTION
Fever is a ubiquitous phenomenon in the intensive care unit.1 Although fever is a natural response to illness and injury, the occurrence of an elevated temperature in a critically ill patient frequently initiates both a gamut of unfocused diagnostic testing and multiple intravenous infusions of broad-spectrum antibiotics, often without a critical appraisal of the unique issues of the individual patient. This “one-size-fits-all” approach may not only add unnecessary costs, manpower, and interventions to patient care but may also expose patients to unnecessary risks. However, in selected patients, clinical pathways have the potential both to reduce costs and to improve the appropriateness of treatment, the latter of which may then lead to improved survival. A thorough understanding of the common etiologies of fever is critical to customizing the care of individual patients. In this chapter, we will review the physiology of temperature regulation, how to best measure temperature in the ICU, the epidemiology and the clinical impact of fever, the differential diagnosis of elevated body temperature, common infectious and noninfectious causes of fever, and general guidelines to evaluation and management in hopes to provide the reader with a rational approach to the febrile patient in the intensive care unit.
TEMPERATURE REGULATION AND MEASUREMENT
Healthy, nonfasting, resting adults, closely regulate sublingual temperature between 33.2°C and 38.1°C.2 There is normally a small normal diurnal variation in temperature of approximately 0.5°C, which nadirs around 6 am and peaks around 4 pm.3 This tight regulation occurs due to continual adjustment of thermogenic and cooling processes. Eating, exercise, and sleep deprivation increase body temperature while fasting reduces it.4 Technically fever refers to an increase in the natural set point for homeostatic temperature control while hyperthermia refers to an uncontrolled elevation of body temperature.
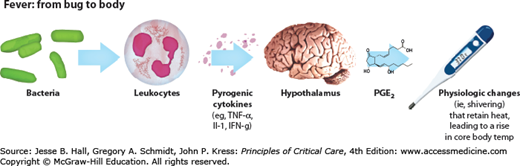
Thermoregulation resides within the hypothalamus.5 While countless exogenous and endogenous pyrogens have been identified, almost all have been shown to stimulate the release of proximal proinflammatory cytokines, such as IL-6, IL-8, IL-1β, and TNF, which subsequently induce the synthesis of prostaglandin E2 (PGE2) within the preoptic nucleus of the anterior hypothalamus (Fig. 63-1). Binding of PGE2 shifts the hypothalamic thermostat increasing sympathetic activity, inducing shivering, and impairing heat loss.6 Typically patients with fever experience chills until the core body temperature rises to the new set point.
Body temperature can be measured by several different methods and at many different sites. The most common clinically used sites are the mouth, axilla, rectum, skin, tympanic membrane, bladder, central veins, and pulmonary artery. Under normal circumstances, rectal temperature is approximately 0.5°C higher and axillary temperature 0.1°C lower than sublingual temperature.2 During critical illness the variability between sites may increase. For example, during open mouth breathing, sublingual temperature falls relative to tympanic membrane temperature.7 Likewise, skin temperature can fall relative to core temperature during cardiogenic shock due to a decrease in cutaneous blood flow. Because of this variability, mouth, skin, and axillary measurements are not recommended for use in critically ill patients.8 Often a rectal probe is recommended because it provides accurate and minimally invasive measurements of core temperature; however, some have suggested that rectal thermometers pose a risk of bacteremia in neutropenic patients.9 Central venous thermistor measurements have long been the gold standard for core temperature measurement, but with the decline in the use of thermodilution pulmonary artery catheters, this method is now rarely used. Whatever the chosen method and the chosen site of measurement, both should be documented and used consistently.
EPIDEMIOLOGY AND IMPACT OF FEVER
Very often fever is the first and only sign of a serious underlying infection while at other times it may simply represent a normal stress response to critical illness. A consensus task force from the American College of Critical Care Medicine and the Infectious Diseases Society of America has defined fever as a single oral temperature of >38.3°C or an oral temperature >38.0°C for at least 1 hour.8 Using this definition, up to 70% of critically ill adults have fever at some time during their ICU stay.10
Although the presence of fever may be an adverse prognostic indicator, animal data support a teleological role for fever during infection; that is, modest elevations in body temperature improve host defenses against infection.11,12 The mechanisms by which fever can favorably affect immunity are diverse. For example, fever can induce the production of heat shock proteins and it can have counter regulatory effects on proinflammatory cytokines.13-15
Along this same theme, the inability to mount a febrile response to infection can be an ominous prognostic sign. Septic patients who experience natural hypothermia (<35.5°C) have a significantly increased risk of death (62% vs 26%) and have higher Sequential Organ Failure Scores (SOFA) when compared to febrile patients.16,17
In spite of the purported beneficial effects of fever, most intensivists correctly associate fever with adverse outcomes. Febrile ICU patients tend to experience more agitation, undergo more laboratory testing, have a longer ICU length of stay, have increased hospital costs, and have higher mortality than patients without fever.10,17-23 In a retrospective cohort of 24,204 ICU admissions, the cumulative incidence of fever was 44%. Fever was more common among patients with trauma or neurological illness, and more common among males and younger patients. Seventeen percent of patients who had fever had positive cultures and those with high fever had an increased risk of death.21 In a second study, up to 1/3 of patients with traumatic brain injury had prolonged fever, which was associated with tachycardia, hypertension, tachypnea, excessive diaphoresis, extensor posturing, or severe dystonia.24 In a third observational study, febrile elderly patients in a medical-surgical ICU had almost twice the risk of agitation than normothermic control patients. And those with higher temperature had a greater risk of severe agitation.
The health care costs of responding to fever are also significant. Nursing time is increased among febrile patients, which can have adverse effects on the allocation of nursing personnel.25 One estimate suggests that fever might add approximately $17,000 in additional costs to the care of critically ill neurological patients and that 3/4 of these costs occur in the ICU.22
DIFFERENTIAL DIAGNOSIS OF FEVER IN THE ICU
The recognition of fever in a critically ill patient often leads to the reflex ordering of blood, sputum, and urine cultures and the initiation of empiric, intravenous, broad-spectrum antibiotics. This shotgun approach can add unnecessary costs and risks to patient care.26 In 2008, a panel composed of members of the Society of Critical Care Medicine and the Infectious Diseases Society of America published a consensus guideline on the recommended management of new onset fever in the ICU population.8 The panel stressed that fever has many noninfectious causes in addition to the usual infectious ones, and, therefore, a careful clinical evaluation should precede laboratory testing, x-rays, and empiric treatment. Consideration of the unique factors of each patient was emphasized over the initiation of routine order sets. This approach should then lead to an individualized differential diagnosis of the potential causes of fever and thereby more focused and cost-effective diagnostic testing.
Common causes of fever in ICU patients are listed in Table 63-1. The prevalence of each of these diagnoses will largely depend on the patient population being studied. For example, benign postoperative fever (surgical trauma) would be overrepresented in a surgical ICU while fever due to stroke would be more commonly seen in a neurointensive care unit.
Common Causes of Fever in Critically Ill Patients
|
|
SELECTED INFECTIOUS CAUSES OF FEVER
The evaluation of fever in the ICU usually begins with a search for signs of infection, since approximately only half of febrile events in the ICU are due to infection and the majority of these infections are related to devices, for example, urinary catheters, endotracheal tubes, nasogastric tubes, or central venous catheters.10 The early removal of devices when they are no longer needed is a very cost-effective strategy for reducing ICU infections and many ICUs now utilize the daily goals checklists on interdisciplinary rounds to document the necessity for each device.
Blood cultures should be obtained from all ICU patients with a new fever when the clinical picture does not strongly suggest a noninfectious cause.8 In order to maximize the sensitivity of blood cultures for true bacteremia, guidelines from the American College of Critical Care Medicine and the Infectious Diseases Society of America8 emphasize that the blood cultures should be obtained prior to antibiotic initiation and that an adequate volume of blood should be instilled into the collection bottles (usually 20-30 mL per culture).27 Spacing out sets of blood cultures over time does not increase the yield. In order to avoid contamination, the blood cultures should be drawn only after proper hand washing and after sterilization of the intended site with an approved individually prepackaged chlorhexidine, alcohol, or iodine-based applicator.
There has been an explosion in the use of central venous catheters in the ICU and with it an increase in risk of central line–associated bloodstream infection (CLABSI). Use of full barrier precautions, shorter duration of catheter use, use of antibiotic impregnated catheters, avoidance of femoral venous access, and care by a central-line team are factors associated with a lower risk of CLABSI.28 Measurement of the “differential time to positivity,” that is, the difference in time for blood cultures to become positive when they are drawn simultaneously through a central venous catheter and a peripheral vein, has been shown to have high sensitivity and specificity for catheter-related infection.29 When line sepsis is suspected, the line should be removed aseptically and 5cm of the line tip submitted for semiquantitative culture. Isolation of ≥15 colony-forming units (CFUs) on semiquantitative culture of the catheter tip correlates with true line-associated infection.30 Isolation of <15 CFUs usually represents contamination during removal. However, it is not recommended to routinely culture line tips upon removal from asymptomatic patients. In one epidemiologic study of intensive care unit-acquired bloodstream infections, multiple antibiotic-resistant organisms were uncommon suggesting it may be safer to use a more narrowed spectrum of antibiotics.31
Urine cultures are almost universally obtained during the evaluation of fever in a critically ill patient regardless of patient age, gender, and duration of catheter placement. However, urinary tract infections in the ICU occur almost exclusively in patients who have had indwelling urinary catheters for a long duration and the infections occur more frequently in females and in those patients who have received prior antibiotics.32 In an 18-month retrospective study of 510 trauma patients, the incidence of urinary tract infections was estimated to be only 16/1000 catheter days, and during the first 2 weeks of urinary catheter use, urinary tract infection was found to be an unlikely cause of either fever or leukocytosis.33
When clinically indicated, most ICU urinary cultures are obtained from an indwelling catheter because very few critically ill patients are candidates for clean catch, midstream specimens. When obtaining cultures from an indwelling catheter, it is paramount to adequately sterilize of the rubber port prior to sampling and to promptly process the specimen in less than 1 hour to prevent bacterial proliferation.8 Cultures should never be obtained from a collection bag. A better idea is to obtain the culture from an “in-and-out” straight catheterization because it avoids contamination of the specimen by bacteria adherent to the indwelling urinary catheter. In rare cases, an ultrasound-guided suprapubic tap can be obtained to avoid contamination from the highly colonized distal urethra.
In a retrospective review of patients undergoing major gynecologic surgery, 80% of patients who developed pneumonia had symptoms suggestive of the diagnosis,34 whereas obtaining a routine chest x-ray on all febrile patients yielded a finding of pneumonia in only 9% of cases. These data would suggest that chest radiography for the evaluation of fever in nonintubated post-op patients should be reserved for patients with signs and symptoms of pneumonia.
Although the performance of routine daily chest x-rays on stable, nonintubated patients in the ICU has a low diagnostic yield for pathology, it is often appropriate to obtain an on-demand chest x-ray in a critically ill, ventilated patient with fever.35,36 The incidence of ventilator-associated pneumonia (VAP) has been reported to range from 5% to 67% among mechanically ventilated patients37 with an attributable mortality of up to 10%.38 In practice, the diagnosis is most often made using readily available clinical variables (eg, characterization of secretions, chest x-ray appearance, body temperature, leukocyte count, culture, and measurement of the <SPAN role=presentation tabIndex=0 id=MathJax-Element-1-Frame class=MathJax_Error style="POSITION: relative" data-mathml='PaO2′>[Math Processing Error]PaO2/<SPAN role=presentation tabIndex=0 id=MathJax-Element-2-Frame class=MathJax_Error style="POSITION: relative" data-mathml='FiO2′>[Math Processing Error]FiO2 ratio). However, it is clear that many intubated patients who meet these clinical criteria do not have VAP.39 Compared to a simple tracheal aspirate and culture, the use of invasive techniques, such as bronchoalveolar lavage, to definitively establish the diagnosis of VAP does not appear to reduce the use of antibiotics nor does it appear to improve clinical outcomes.40 The preferred approach when VAP is suspected is to initiate empiric broad-spectrum antibiotics using existing guidelines41 followed by rapid de-escalation of broad-spectrum antibiotics based on culture results.42
Most ICU patients will at some point have an endotracheal tube, a nasogastric tube, or a nasotracheal suctioning device. These indwelling tubes can cause mucosal trauma, introduce bacteria, and promote biofilm formation all of which increase the likelihood of infection and fever. Within 1 week of nasotracheal intubation and nasogastric tube placement, approximately 1/3 of patients will have purulent maxillary sinusitis, a rate approximately fourfold greater than that associated with oral placement.43
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


