PENETRATING TRAUMA
CASE SCENARIO
A 25-year-old man is brought the emergency room by emergency medical services (EMS) directly from the scene of a shooting. On arrival in the trauma bay he is awake and confused, but protecting his airway. He has decreased breath sounds on the right side, and a palpable femoral pulse. His vital signs are significant for tachycardia to 140, a blood pressure of 90/40, tachypnea, and an oxygen saturation of 88% on 4-L nasal cannula. A chest film shows a right-sided hemopneumothorax. A tube thoracostomy is performed with return of air and 500 cc of blood, and improvement in his mental status and vital signs.
A complete secondary survey reveals a laceration to his right lateral neck, and gunshot wounds to the right axilla and right thigh. He has right anterior chest crepitus, and a large non-pulsatile hematoma in his right thigh.
EPIDEMIOLOGY
Trauma is a major leading cause of death in the United States and the world. Worldwide, injuries are the fifth leading cause of death overall, and the leading cause of death in those under 35 years of age.1 In 2011, nearly 5 million people worldwide died from traumatic injuries, compared with 6.8 million from all infectious diseases.2 In the United States, trauma is the fifth leading cause of death,3 and is the leading cause of death among individuals aged 1 to 44 years.
While penetrating trauma usually constitutes only 15% of injuries incurred in the civilian sector, in some urban centers in the United States, this fraction approaches 20% to 45%.1,4 Although the incidence of stabbings and gunshots has decreased in the United States,4 higher rates of gun ownership have been associated with higher rates of suicide by firearm.5 The injury pattern of penetrating trauma tends toward more severe thoracoabdominal injuries than in blunt trauma, and about 90% of injuries to the great vessels of the thorax are caused by penetrating trauma.1 In addition, while less than 20% of deaths in blunt trauma are due to bleeding, nearly half of patients with lethal penetrating injuries bleed to death.4
PATHOPHYSIOLOGY
The pathophysiology of penetrating trauma depends on the energy of the injury and the type of projectile. In a study of injuries from the 1991 Gulf War, shrapnel injuries all affected soft tissue, one third caused bony injury, and only 10% caused abdominal or thoracic visceral injury.6 A stab wound imparts relatively little energy, and injury depends on the size of the weapon used. The wounding potential of bullets depends on velocity, caliber, and whether the bullet expands or not (i.e., whether or not it is jacketed). The bullet mass determines the penetration depth of the bullet, and bullet shape determines trajectory through tissues. Tissue factors, including elasticity and density, determine how the tissue will respond to temporary cavitation.7 While full-metal jacket bullets may cause deeper penetration into tissues, hollow-point bullets that expand on entry can impart more energy to tissues, causing more tissue destruction.8 A high-speed rifle bullet, if it wounds an extremity without hitting bone, may cause minimal injury as the bullet leaves the body without expending much energy. For these reasons, hollow-point bullets from low-velocity weapons—such as pistols—may inflict more damage to tissue than full-metal jacket rounds from a rifle. However, once in the torso, these full-metal jacket bullets can yaw so that they pass through tissue sideways and cause significant tissue destruction.7
The most important factor in the pathophysiology of penetrating trauma is location. A small stab wound to the heart may cause a far more lethal injury than a high-velocity rifle round through thigh musculature.
CLINICAL PRESENTATION
Clinical presentation depends on the location of injury and the timing. Approximately 50% of severely injured trauma patients will die either on the scene or en-route to the hospital. Of those who survive to present to the hospital, about 50% will die within the first 24 hours—mostly of exceedingly severe injuries, i.e., catastrophic brain injury, or massive blood loss.9
The remainder of the chapter categorizes injuries by anatomical location, as the workup and management varies depending on the structures involved.
 Neck
Neck
When considering penetrating injuries, the neck is anatomically described as consisting of anterior and posterior triangles, divided by the sternocleidomastoid. The anterior triangle is further divided into 3 zones: Zone I, sternal notch to cricoid cartilage; Zone II, cricoid cartilage to angle of mandible; Zone III, superior to the angle of the mandible10 (Figure 31–1). On the other hand, some neck wounds can be difficult to classify by zone, and the skin wound may not reflect underlying damage. For these reasons, injuries to the neck may be more helpfully divided into a few clinical groups that predict the need for operative repair: airway compromise; isolated laryngotracheal injuries; carotid, jugular, pharyngeal, and esophageal injuries; wounds at the base of the neck; vertebral artery injuries; and superficial wounds.11 While wounds that present with airway compromise secondary to compressive hematoma may be dramatic, isolated laryngotracheal injuries can be more subtle, and present only with subcutaneous emphysema or hoarseness.12 Injuries to the vascular structures will present with hematomas, which may expand and have an associated bruit in the case of a carotid injury.12 Pharyngeal and esophageal injuries present with subcutaneous emphysema, dysphagia, odynophagia, or hematemesis.12 Wounds at the base of the neck (Zone I) should elicit a high suspicion for extension into the thorax, and an injury to the posterior triangle of the neck with ongoing hemorrhage suggests a vertebral artery injury.11 Superficial wounds that do not violate the platysma, in contrast, incur little injury and require no further workup.12
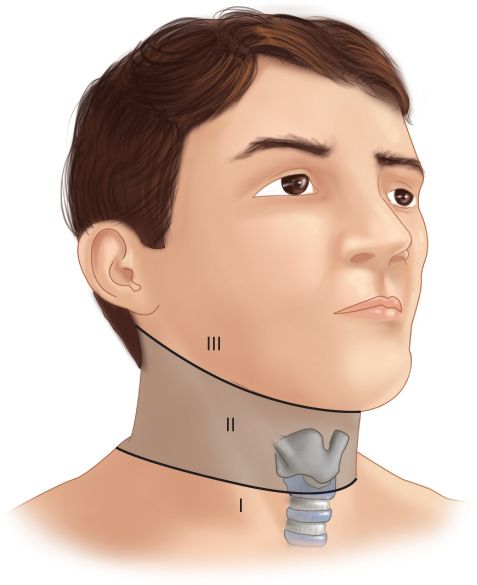
Figure 31–1 Zones of the neck for penetrating trauma. Zone I is from the suprasternal notch to the cricoid cartilage; Zone II from the cricoid to the angle of the mandible; and Zone III above the angle of the mandible. (Reproduced with permission from Brunicardi FC, Andersen DK, Biliar TR, Dunn DL, Hunter JG, Matthews JB, Pollack RE: Schwartz’s Principles of Surgery, 10th Edition. New York, NY: McGraw-Hill;2015.)
 Thorax
Thorax
Major injuries to the thorax may be divided into 14 types: the “lethal six” that must be identified immediately, and the “hidden eight” that can be more subtle and should be diagnosed during the secondary survey.13 The “lethal six” include (1) airway obstruction, (2) tension pneumothorax, (3) open pneumothorax, (4) flail chest, (5) massive hemothorax, and (6) cardiac tamponade. The “hidden eight” include (1) simple pneumothorax, (2) hemothorax, (3) pulmonary contusion, (4) tracheobronchial injury, (5) blunt cardiac injury, (6) traumatic aortic disruption, (7) traumatic diaphragmatic injury, (8) esophageal injury. The most common location of esophageal injury is in the cervical esophagus and is discussed above.13 In order to focus on penetrating trauma we focus our discussion herein to tension pneumothorax, open pneumothorax, massive hemothorax, and cardiac tamponade.
Tension pneumothorax, massive hemothorax, and cardiac tamponade all present with shock and chest pain. Hypoxemia and shock combined with a unilateral absence of breath sounds may reflect either tension pneumothorax or massive hemothorax. A tension pneumothorax may be differentiated by hyper-resonance to chest percussion and tracheal deviation, whereas a massive hemothorax will present with dullness to percussion. Both tension pneumothorax and cardiac tamponade may present with distended neck veins.13
Open pneumothoraces are typically caused by high-velocity missiles fired at close range, and are characterized by a large wound across which atmospheric and intrathoracic pressure equilibrate. If the wound is more than two-thirds the diameter of the trachea, air will preferentially enter the thorax through the wound rather than the trachea, precipitating lung collapse and compromising ventilation.13
 Abdomen
Abdomen
The majority of abdominal gunshot wounds cause significant intra-abdominal injury and mandate exploratory laparotomy. In contrast, only 20% to 30% of stab wounds inflict significant damage, and should be locally probed in the stable patient. If a stab wound violates the anterior rectus sheath, laparotomy may be indicated.14 Recent studies have questioned the need for mandatory exploration in penetrating abdominal trauma, and selective nonoperative management may be practiced in the hemodynamically stable patient without signs of peritonitis or signs of hollow viscus injury on imaging.15,16 The liver and small bowel are the most commonly injured organs in penetrating injury to the abdomen.
 Extremities
Extremities
Penetrating trauma to the extremities may cause injury to soft tissues, bones, vasculature, or a combination of all three. Penetrating vascular injury may either transect the vessel partially or completely. A completely transected vessel may cause vasospasm or thrombosis, whereas a partial transection may continue to bleed, especially with resuscitation.17
Physical examination of patients with vascular injuries may reveal two classes of findings. Hard signs of vascular injury include arterial bleeding, ongoing hemorrhage with shock, expanding or pulsatile hematoma, palpable thrill, absent distal pulses, or limb ischemia. Such findings reflect life- or limb-threatening injury, and necessitate immediate operative exploration and repair. Soft signs of vascular injury include severe hemorrhage at the scene, non-expanding and non-pulsatile hematomas, unequal pulses or Ankle brachial indices (ABIs), and neurologic deficits. Patients with soft signs of vascular injury do not require immediate operative exploration; however, their presentation mandates expeditious and thorough diagnostic evaluation.17,18
DIFFERENTIAL DIAGNOSIS
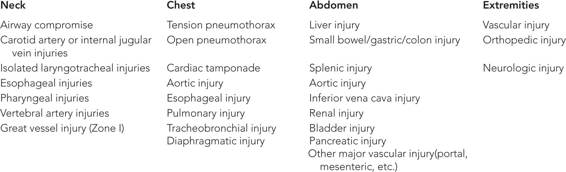
Differential diagnosis depends on the trajectory, location, and mechanism of the injury. In general, missiles take a straight course, damaging organs and vessels in a vector from entry wound to exit wound. In the case of stabbings, the extent of injury depends on the depth to which the weapon has penetrated the abdomen or thorax (Table 31–1).
WORKUP AND CHOICE OF IMAGING
The workup and initial treatment of any trauma patient proceeds according to the Advanced Trauma Life Support (ATLS) guidelines. Workup and initial management involves the primary and secondary survey. The primary survey follows the ABCDE mnemonic: Airway, Breathing, Circulation, Disability, and Exposure. Following this, a complete physical examination, the secondary survey, is performed to fully evaluate for all injuries. Adjuncts to the primary survey—to be obtained prior to the secondary survey in an unstable patient—include chest x-ray, pelvic x-ray, and, in blunt trauma, the focused assessment with sonography for trauma (FAST) examination.19
 Neck
Neck
In the case of penetrating trauma to the neck, particular attention is paid to the airway and vessels. In the case of a gurgling wound or pulsatile or growing hematoma, the airway is secured and the patient taken directly to the operating room. However, in the absence of obvious signs of vascular or airway injury, the appropriate workup is determined by the location of the injury. Studies show that ultrasound examination is unreliable for diagnosis of vascular injury of the neck. Computed tomography angiography (CTA) is the preferred modality, with a negative predictive value of 97% to 100%.20 Furthermore, CTA can characterize the wound track and assist with operative planning if necessary. In the case of a Zone I injury, CTA cuts should extend into the chest to evaluate for injuries to the great vessels, airway, and esophagus. In a Zone III injury, CTA of the neck extending up to the skull base is performed to evaluate the pharynx and vessels of the upper neck. While the classical teaching requires immediate exploration for Zone II neck injuries, the stable patient may be observed with a CTA and triple endoscopy (esophagoscopy, bronchoscopy, laryngoscopy) to evaluate for injuries to the pharynx, trachea, esophagus, and vessels of the neck.21
 Chest
Chest
Penetrating trauma to the chest is first evaluated with chest x-ray as an adjunct to the ATLS primary survey. Hemoor pneumothorax is evacuated with tube thoracostomy. Massive hemothorax (>1500 cc on placement or >2000 cc over 4 hours) mandates immediate operation. In the case of a normal chest x-ray, the stable patient may be observed with a repeat chest x-ray in 3 to 4 hours. If the plain film continues to be normal, the patient may be safely discharged. Diagnosis of cardiac injury may be assisted by the sub-xyphoid view of a FAST examination. Evidence of pericardial effusion suggests cardiac injury until proven otherwise.
Penetrating trauma, especially transmediastinal gunshot wounds, also risks injury to the great vessels, the airway, and the esophagus. Such a mechanism requires a high level of suspicion for life-threatening injury, as crowding of vital structures in the mediastinum permits devastating trauma with a single projectile. Unstable patients require immediate operative exploration. Stable patients, however, should undergo CTA for initial evaluation of great vessel injury, followed by esophagogram to rule out esophageal injury.22 Persistent air leak from a chest tube suggests possible airway injury, and should be followed up with bronchoscopy in the operating room (OR). CT can also assist in the diagnosis of tracheobronchial or esophageal injury; however, it does not preclude the need for bronchoscopy and esophagoscopy to definitively rule out aerodigestive tract injury.
 Thoracoabdominal
Thoracoabdominal
Penetrating injuries to the diaphragm may be difficult to diagnose, as diaphragmatic defects are usually small. A high index of suspicion is warranted, as up to 36% of patients with thoracoabdominal stab wounds may have diaphragmatic injury.23 The gold standard for the diagnosis of diaphragmatic injury is thoracoscopy or laparoscopy, which may be therapeutic as well as diagnostic and obviate the need for laparotomy.23,24 Multi-detector CT has been shown to have a sensitivity up to 87% for detection of diaphragmatic injuries; however, imaging can confer little information about defect location and size.25 A small study using intrapleural gastrograffin (infused through a chest tube) showed 100% sensitivity and 94% specificity, although this is not standard of care.26 The most helpful signs of potential diaphragmatic injury are contiguous organ injury, pleural effusion, air tracking below the diaphragm, or a wound tract extending up to the diaphragm.27
 Abdomen
Abdomen
Unstable patients with penetrating wounds to the abdomen require immediate operative exploration, and no time should be wasted in obtaining imaging studies. In hemodynamically stable patients with stab wounds to the abdomen, however, local wound exploration to determine fascial penetration can dictate management. Chest x-ray in thoracoabdominal trauma can rule out injury to the chest, and oftentimes, the scout film from a CT can clarify the location and path of the projectile, which in turn assists in determining which organs are injured. CT with IV contrast can elucidate renal or retroperitoneal injury, as well as injury to the inferior vena cava (IVC) or aorta. Evaluation of penetrating trauma to the pelvis may be assisted with triple-contrast CT scan (oral/IV/rectal) to further evaluate for rectal injuries.14,27
 Extremity
Extremity
The traditional modality for diagnosis of extremity vascular injury is angiography; however, in the modern era this technique is invasive, time-consuming, overly sensitive, and not cost-effective.17 In most patients, evaluation begins with a thorough neurovascular examination. In patients with abnormal ankle-brachial reflexes, peripheral neurologic deficits, or asymmetric pulse examinations, CTA is highly sensitive (95%–100%) and specific (87%–100%) for diagnosis of extremity vascular injury, and should be the first imaging study.20
IMAGING FINDINGS
 Penetrating Neck Trauma
Penetrating Neck Trauma
CT Scan
Within the neck, the CTA imaging findings of particular import are those that suggest injury to blood vessels or the aerodigestive tract. Vascular injury may appear as active extravasation, or, more subtly, a pseudoaneurysm, which will appear as a round collection of hyperdense contrast arising from an artery. Aerodigestive tract injury will appear as subcutaneous emphysema, or hypodense air appearing in a location outside the defined borders of the trachea and esophagus. Subcutaneous emphysema can be best appreciated by switching to lung windows. Any air anterior to the trachea or posterior to the esophagus is abnormal.
While CTA is sensitive for esophageal injuries, contrast esophagram (in the non-intubated patient) and esophagoscopy are more sensitive. These studies should be performed if there is any suspicion of esophageal injury, as the mortality of esophageal injury increases as the time from injury to repair increases21 (Table 31–2 and Figures 31–2 and 31–3).







