CHAPTER 174
Pediculosis
(Lice, Crabs)
Presentation
Patients arrive with emotions ranging from annoyance to sheer disgust at the discovery of an infestation with lice or crabs and request acute medical care. There may be extreme pruritus, and the patient may bring in a sample of the creature to show you. Head lice generally affect children, primarily girls, aged 3 to 12 years. The adult forms of head lice can be very difficult to find, but their oval, light gray eggs (nits) can be readily found firmly attached to the hairs above the ears and toward the occiput. Secondary impetigo and furunculosis can occur.
The adult forms of pubic lice (Phthirus organisms or crab lice) are more easily found, but their light yellow-gray color still makes them difficult to see. Small black dots present in infested areas represent either ingested blood in adult lice or their excreta. Maculae ceruleae (bluish-brown macules), which represent intradermal hemorrhage at sites where lice have fed, can sometimes be found. Pubic lice are not limited to the pubic region and may be found on other short hairs of the body, such as body hair, eyebrows, and eyelashes (pediculosis ciliaris).
Identification of lice, larvae, or viable nits with a magnifying glass makes the diagnosis (Figure 174-1).
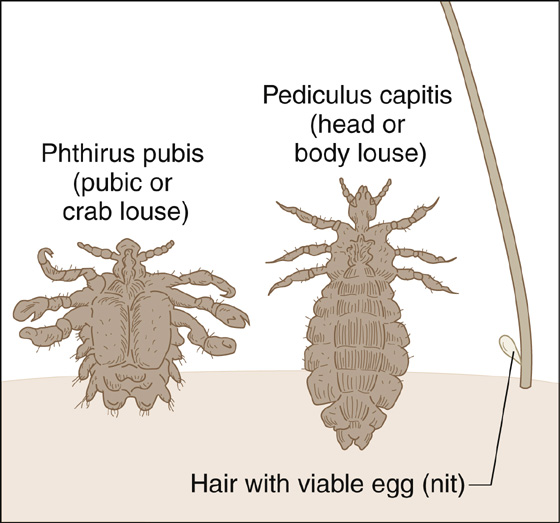
Figure 174-1 Pediculosis.
What To Do:
 For head lice, instruct the patient and other close contacts regarding the use of nonprescription louse treatments. The most effective is 1% permethrin (Nix), which should be applied undiluted to clean, towel-dried hair until the affected area is entirely wet. After 10 minutes, shampoo and rinse with warm water. It is not necessary to remove nits. To kill newly hatched nymphs, a second treatment should be given 7 to 10 days later.
For head lice, instruct the patient and other close contacts regarding the use of nonprescription louse treatments. The most effective is 1% permethrin (Nix), which should be applied undiluted to clean, towel-dried hair until the affected area is entirely wet. After 10 minutes, shampoo and rinse with warm water. It is not necessary to remove nits. To kill newly hatched nymphs, a second treatment should be given 7 to 10 days later.
 Itching or mild burning of the scalp caused by inflammation of the skin in response to topical therapeutic agents can persist for many days after lice are killed, and the condition is not a reason for re-treatment. Topical corticosteroids and oral antihistamines may be beneficial for relieving these signs and symptoms.
Itching or mild burning of the scalp caused by inflammation of the skin in response to topical therapeutic agents can persist for many days after lice are killed, and the condition is not a reason for re-treatment. Topical corticosteroids and oral antihistamines may be beneficial for relieving these signs and symptoms.
 For severe or resistant infestations, combining 1% permethrin treatment with oral trimethoprim/sulfamethoxazole (TMP/SMX), 5 mg/kg bid for 10 days, will have a higher cure rate than permethrin alone at 4 weeks (93% vs. 72%). TMP/SMX is not toxic to the louse; instead, it acts by killing essential bacterial flora in the insect’s gastrointestinal tract.
For severe or resistant infestations, combining 1% permethrin treatment with oral trimethoprim/sulfamethoxazole (TMP/SMX), 5 mg/kg bid for 10 days, will have a higher cure rate than permethrin alone at 4 weeks (93% vs. 72%). TMP/SMX is not toxic to the louse; instead, it acts by killing essential bacterial flora in the insect’s gastrointestinal tract.
 A second over-the-counter (OTC) choice is a preparation combining piperonyl butoxide and pyrethrin extracts (RID), which is applied in the same fashion. This product does not kill all of the unhatched eggs and has no residual activity, is less effective, and is more allergenic than permethrin.
A second over-the-counter (OTC) choice is a preparation combining piperonyl butoxide and pyrethrin extracts (RID), which is applied in the same fashion. This product does not kill all of the unhatched eggs and has no residual activity, is less effective, and is more allergenic than permethrin.
 As lice have become resistant to OTC treatments, some clinicians have had to escalate to prescription strength 5% permethrin cream (Elimite) applied to clean, dry hair and left on overnight (8 to 14 hours) under a shower cap. Resistance still occurs even at these higher concentrations of permethrin.
As lice have become resistant to OTC treatments, some clinicians have had to escalate to prescription strength 5% permethrin cream (Elimite) applied to clean, dry hair and left on overnight (8 to 14 hours) under a shower cap. Resistance still occurs even at these higher concentrations of permethrin.
 Benzyl alcohol lotion 5% (Ulesfia [Sciele Pharma, Atlanta, Ga.]) is a prescription medicine that was approved by the U.S. Food and Drug Administration (FDA) in April 2009 for treatment of head lice in children older than 6 months. The product is not neurotoxic and kills head lice by asphyxiation. Patients receive two 10-minute treatments 1 week apart, but consideration should be given to re-treating in 9 days or using three treatment cycles (days 0, 7, and 13 to 15).
Benzyl alcohol lotion 5% (Ulesfia [Sciele Pharma, Atlanta, Ga.]) is a prescription medicine that was approved by the U.S. Food and Drug Administration (FDA) in April 2009 for treatment of head lice in children older than 6 months. The product is not neurotoxic and kills head lice by asphyxiation. Patients receive two 10-minute treatments 1 week apart, but consideration should be given to re-treating in 9 days or using three treatment cycles (days 0, 7, and 13 to 15).
 Resistant infestations with treatment failures are most commonly treated with the prescription formula of malathion (Ovide) 0.5% lotion. Apply it to dry hair and then shampoo. It may be reapplied 7 to 9 days later if necessary. Although a lengthy application time is specified on the product’s label (8 to 12 hours), a recent study found that malathion 0.5% was 98% effective with just one or two 20-minute applications. Because of potential flammability, patients should be instructed to avoid using a hair dryer or curling iron during treatment with malathion. Malathion can only be used in people who are 24 months of age or older, when resistance to permethrin or pyrethrins is documented, or when treatment with these products fails despite their correct use.
Resistant infestations with treatment failures are most commonly treated with the prescription formula of malathion (Ovide) 0.5% lotion. Apply it to dry hair and then shampoo. It may be reapplied 7 to 9 days later if necessary. Although a lengthy application time is specified on the product’s label (8 to 12 hours), a recent study found that malathion 0.5% was 98% effective with just one or two 20-minute applications. Because of potential flammability, patients should be instructed to avoid using a hair dryer or curling iron during treatment with malathion. Malathion can only be used in people who are 24 months of age or older, when resistance to permethrin or pyrethrins is documented, or when treatment with these products fails despite their correct use.
 Removal of all topical pediculicides should be accomplished by rinsing the hair over a sink rather than in the shower or bath. This limits skin exposure. Using warm, rather than hot water, will minimize absorption attributable to vasodilation.
Removal of all topical pediculicides should be accomplished by rinsing the hair over a sink rather than in the shower or bath. This limits skin exposure. Using warm, rather than hot water, will minimize absorption attributable to vasodilation.
 For head lice that are resistant to all other treatments, give a single oral dose of ivermectin (Stromectol), 200 to 400 µg/kg PO once, repeated once after 7 to 10 days. Most recently, a single oral dose of 400 µg/kg repeated in 7 days has been shown to be more effective than 0.5% malathion lotion. Ivermectin should not be used for children who weigh less than 15 kg.
For head lice that are resistant to all other treatments, give a single oral dose of ivermectin (Stromectol), 200 to 400 µg/kg PO once, repeated once after 7 to 10 days. Most recently, a single oral dose of 400 µg/kg repeated in 7 days has been shown to be more effective than 0.5% malathion lotion. Ivermectin should not be used for children who weigh less than 15 kg.
 Instruct families to disinfect sheets and clothing by machine washing in hot water, machine drying on the hot cycle for 20 minutes, ironing, dry cleaning, or just storing in plastic bags for 2 weeks. Combs and brushes should be soaked in 2% Lysol or heated in water to about 65° C for 10 minutes.
Instruct families to disinfect sheets and clothing by machine washing in hot water, machine drying on the hot cycle for 20 minutes, ironing, dry cleaning, or just storing in plastic bags for 2 weeks. Combs and brushes should be soaked in 2% Lysol or heated in water to about 65° C for 10 minutes.
 Nit removal is recommended for aesthetic reasons and can help identify if there is a later recurrence. Removal of the eggs is not necessary to prevent spreading the infestation. Application of a 1:1 solution of white vinegar and water may help to loosen nits before removal with a fine-toothed comb.
Nit removal is recommended for aesthetic reasons and can help identify if there is a later recurrence. Removal of the eggs is not necessary to prevent spreading the infestation. Application of a 1:1 solution of white vinegar and water may help to loosen nits before removal with a fine-toothed comb.
 Pubic lice are most commonly sexually transmitted, and sexual contacts must also be treated. In addition, this finding should prompt an evaluation for other sexually transmitted diseases. Treatment is the same as that for pediculosis capitis, with the exception that pediculosis of the eyelashes should be treated with an occlusive ophthalmic ointment applied to the eyelid margins for 10 days.
Pubic lice are most commonly sexually transmitted, and sexual contacts must also be treated. In addition, this finding should prompt an evaluation for other sexually transmitted diseases. Treatment is the same as that for pediculosis capitis, with the exception that pediculosis of the eyelashes should be treated with an occlusive ophthalmic ointment applied to the eyelid margins for 10 days.
 Patients often want to use “natural,” less toxic products or techniques for their children or themselves. Some occlusive products, such as petroleum jelly (Vaseline), mayonnaise, and olive oil, have been used in place of traditional pediculicides, but their effectiveness has not been established in controlled trials. One OTC product, HairClean 1-2-3, consisting of anise oil, ylang ylang oil, coconut oil, and isopropyl alcohol, was more effective than 1% permethrin in an uncontrolled study.
Patients often want to use “natural,” less toxic products or techniques for their children or themselves. Some occlusive products, such as petroleum jelly (Vaseline), mayonnaise, and olive oil, have been used in place of traditional pediculicides, but their effectiveness has not been established in controlled trials. One OTC product, HairClean 1-2-3, consisting of anise oil, ylang ylang oil, coconut oil, and isopropyl alcohol, was more effective than 1% permethrin in an uncontrolled study.
 A “nonneurotoxic” suffocation-based pediculicide (“Nuvo lotion,” which is actually Cetaphil Gentle Skin Cleanser) produced a high cure rate in children with head lice in one small nonblinded study.
A “nonneurotoxic” suffocation-based pediculicide (“Nuvo lotion,” which is actually Cetaphil Gentle Skin Cleanser) produced a high cure rate in children with head lice in one small nonblinded study.
 One author is an enthusiastic advocate of the LiceGuard Robi Comb, a fine-toothed metal comb that is connected to a single AA battery. When used on dry hair for 5 to 10 minutes daily for 2 weeks, it is said to eliminate head lice by essentially electrocuting them.
One author is an enthusiastic advocate of the LiceGuard Robi Comb, a fine-toothed metal comb that is connected to a single AA battery. When used on dry hair for 5 to 10 minutes daily for 2 weeks, it is said to eliminate head lice by essentially electrocuting them.
 When cosmetically acceptable, head shaving is effective.
When cosmetically acceptable, head shaving is effective.
 When one is facing a persistent case of lice, several explanations must be considered, including misdiagnosis, noncompliance with treatment protocol, reinfestation, lack of adequate ovicidal properties of the treatment product, and resistance to the pediculicide. All household members should be checked for lice, but only those with live lice or eggs within 1 cm of the scalp should be treated.
When one is facing a persistent case of lice, several explanations must be considered, including misdiagnosis, noncompliance with treatment protocol, reinfestation, lack of adequate ovicidal properties of the treatment product, and resistance to the pediculicide. All household members should be checked for lice, but only those with live lice or eggs within 1 cm of the scalp should be treated.
What Not To Do:
 Do not mistake a hair cast for a nit (which is firmly attached to a hair shaft). Hair casts are freely movable along the hair shaft.
Do not mistake a hair cast for a nit (which is firmly attached to a hair shaft). Hair casts are freely movable along the hair shaft. Do not apply pediculicides to wet hair. Water dilutes the product and protects lice as they reflexively close their respiratory spiracles when exposed to water.
Do not apply pediculicides to wet hair. Water dilutes the product and protects lice as they reflexively close their respiratory spiracles when exposed to water.
 Do not recommend comprehensive cleaning of the whole house. Adult lice cannot survive for more than 1 day if they cannot find a meal of blood.
Do not recommend comprehensive cleaning of the whole house. Adult lice cannot survive for more than 1 day if they cannot find a meal of blood.
 Do not have the family use commercial sprays (R&C Spray or Li-Ban Spray) to control lice on inanimate objects. Their use is no more effective than vacuuming.
Do not have the family use commercial sprays (R&C Spray or Li-Ban Spray) to control lice on inanimate objects. Their use is no more effective than vacuuming.
 Do not prescribe lindane (Kwell) shampoo. It is an organochloride compound that is absorbed and can be toxic to the central nervous system and cause anemia. In view of reports of lindane resistance and the availability of products with more favorable safety profiles, it is no longer recommended.
Do not prescribe lindane (Kwell) shampoo. It is an organochloride compound that is absorbed and can be toxic to the central nervous system and cause anemia. In view of reports of lindane resistance and the availability of products with more favorable safety profiles, it is no longer recommended.
 Do not use flammable or toxic substances, such as gasoline or kerosene.
Do not use flammable or toxic substances, such as gasoline or kerosene.
 Do not use products intended for animal use.
Do not use products intended for animal use.
Discussion
Blood-sucking lice have long been successful obligate parasites of humans. The three major lice that infest humans are Pediculus humanus capitis (head louse) (Figure 174-2), Pthirus pubis (crab louse) (Figure 174-3), and Pediculus humanus humanus (body louse). Patients with louse infestation present with pruritus, excoriations, and lymphadenopathy. A hypersensitivity rash, or pediculid, may mimic a viral exanthem.

Figure 174-2 Identifying characteristics of a head louse. (Adapted from Ko CJ, Elston DM: Pediculosis, J Am Acad Dermatol 50:1-12, 2004.)
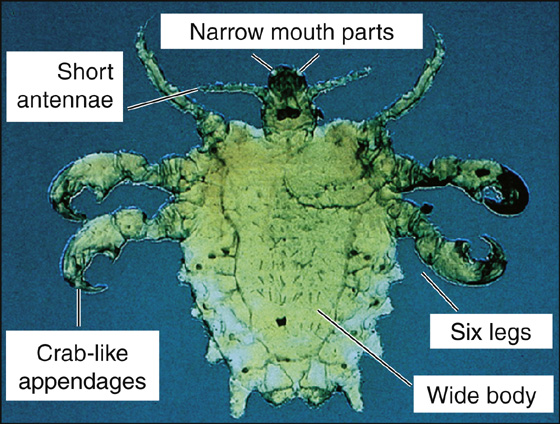
Figure 174-3 Identifying characteristics of crab louse. (Adapted from Ko CJ, Elston DM: Pediculosis, J Am Acad Dermatol 50:1-12, 2004.)
Head lice infestation crosses all economic and social boundaries. The head louse is the size of a sesame seed, 1 to 2 mm in length. After attaching to the patient, the louse inserts its mouth parts and injects saliva with vasodilatory properties. An inflammatory reaction to injected louse saliva has been suggested as the most likely cause of bite reactions. Transmission in most cases occurs by direct contact with the head of another infested individual. Head lice move by grasping hairs, generally remaining close to the scalp. Head lice can crawl rapidly, traveling up to 23 cm/min. Lice egg cases are referred to as nits. They are firmly cemented to human hair and are thus difficult to remove (Figure 174-4). Except in very humid climates, lice lay nits (ova within a chitinous case) within 1 to 2 mm of the scalp. Young lice hatch within 1 week and pass through three nymphal stages, maturing to adults over a period of 1 week. Lice must generally eat every 4 to 6 hours. In most climates, they survive only several hours off the scalp, although they may live for up to 4 days in favorable conditions. In the United States, blacks have a lower incidence of infestation, possibly because lice are better adapted to grasp the more cylindrical hairs of whites or Asians.

Figure 174-4 Lice nit firmly cemented to human hair. (Adapted from Ko CJ, Elston DM: Pediculosis, J Am Acad Dermatol 50:1-12, 2004.)
The diagnosis of head lice is definitive when crawling lice are seen in the scalp hair or are combed from the scalp. Because head lice avoid light and can crawl quickly, the use of louse combs increases the chances of finding live lice. Nits alone are not diagnostic of active infestation, but if the nits are within 1 cm (¼ inch) of the scalp, active infestation is likely. Hair casts may closely resemble nits stuck to hair shafts. A parent, teacher, or school nurse generally notices them and mistakes them for nits. In contrast to nits, hair casts are freely movable along the hair shaft. Among presumed “lice” and “nits” submitted by physicians, nurses, teachers, and parents to a laboratory for identification, many were found to be artifacts such as dandruff, hairspray droplets, scabs, dirt, or other insects (e.g., aphids blown by the wind and caught in the hair).
The female louse lives about 3 to 4 weeks and lays approximately 10 eggs a day. The eggs are incubated by body heat and hatch in 7 to 10 days. If newly hatched eggs that survived the initial therapy are not re-treated, the cycle may repeat itself every 3 weeks.
Although there is no proven transmission from fomites, such as brushes, hats, combs, linens, and stuffed animals, head lice and ova have been found on such items; therefore it is probably expedient to eradicate these lice by vacuuming, washing, dry cleaning, or isolating items in sealed plastic bags for 2 weeks. These insects do not hop, jump, or fly.
No healthy child should be excluded from or allowed to miss school time because of head lice. “No nit” policies for return to school should be discouraged.
Pubic lice are distinct in appearance from head and body lice; they have short crablike bodies. They are challenging to eradicate, because they often inhabit several hair areas on an individual patient (Figure 174-5). A major concern in treating crab lice is the lack of appreciation for their tendency to reside in rectal hairs. If one treats patients with P. pubis with topical preparations, one must instruct patients to liberally treat the groin and rectal regions; otherwise, treatment failures will occur. Some dermatologists prefer to treat pubic lice using ivermectin as their first-line therapy. Besides sexual transmission, pubic lice may also be acquired by sharing a bed with an infested person. Children with pubic lice have usually been infected through contact with an adult. Always demand investigation for possible child abuse.
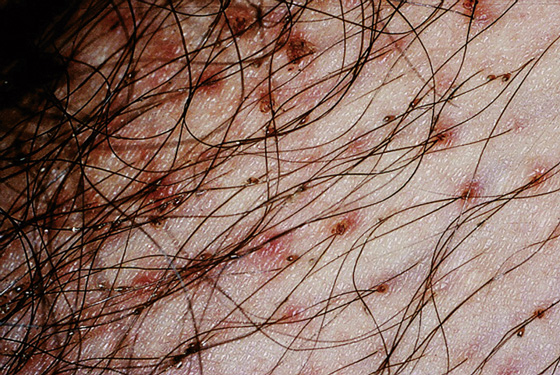
Figure 174-5 Crab louse nits at the base of lower abdominal hairs. (Adapted from Ko CJ, Elston DM: Pediculosis, J Am Acad Dermatol 50:1-12, 2004.)
Fortunately, head and pubic lice do not transmit systemic disease.
In the United States, the body louse has become less common in the general population. Body lice infestation in all developed countries is generally seen among the homeless in urban areas. It also is common among refugees and those who live in crowded conditions or cannot launder their clothing. Worldwide, body lice are important vectors for louse-borne relapsing fever, trench fever, and epidemic typhus, especially among refugees. The body louse and nits are generally found in the clothing seams of a parasitized individual, but the louse grabs onto body hairs to feed. Clothing may be stained with serum, blood, or louse feces. Body lice are eradicated by means of proper hygiene and laundering of clothing. A pediculicide may be helpful to treat any lice adherent to body hairs.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


