CHAPTER 30 PAIN IN CHILDREN
4. What myths have complicated our management of children’s pain?
The following myths have complicated our management of children’s pain:





5. How do you assess pain in infants?
Several pain scales that can be used for children, including infants (Table 30-1 and Figs. 30-1 and 30-2), comprised of itemized lists of the various distress behaviors, have been designed to more specifically assess pain intensity. Clinicians complete these scales by observing infants for a specified period, noting which behaviors occur, and ranking their intensity on a 0-4 scale. The greater the number and intensity of distress signals, the greater the pain level.
TABLE 30-1. Verbal Descriptor Scales To Assess Pain Intensity For Children
| Pain Intensity for Children 7 Years of Age and Older | Pain Intensity for Children Younger Than 7 Years of Age |
|---|---|
| No pain | None |
| Mild pain | A little bit |
| Moderate pain | A medium amount |
| Strong pain | A lot |
| Intense pain | A real lot |
Figure 30-1 Facial affective scale to assess pain affect.
(From McGrath PA: Pain in children: nature, assessment and treatment, New York, 1990, Guilford Press, with permission.)


6. How do you assess pain in children?
By the age of 5, most children can differentiate a wider range of pain intensities and can use many analogue, facial, and verbal rating scales (see Figs. 30-1 and 30-2) to indicate the strength of their pain. Children choose a level on the scale that best matches the strength of their own pain. These scales are easy to administer, requiring only a few seconds once children understand how to use them. Many of these scales yield pain scores on a scale of 0 to 10.
9. Is there a basic treatment algorithm that covers pain control in children?
Yes. There is a basic treatment algorithm that covers pain control in children. It provides a brief summary of the steps to controlling pain in children (Fig. 30-3). The first step is to assess the child with pain, evaluating not only the primary sensory characteristics of the pain (its quality, intensity, location, duration, and aversive component) but also the extent to which situational factors (cognitive, behavioral, and emotional) may be influencing the child’s pain. Direct appropriate physical and medical examinations not only at the primary source of pain but also at secondary sources.
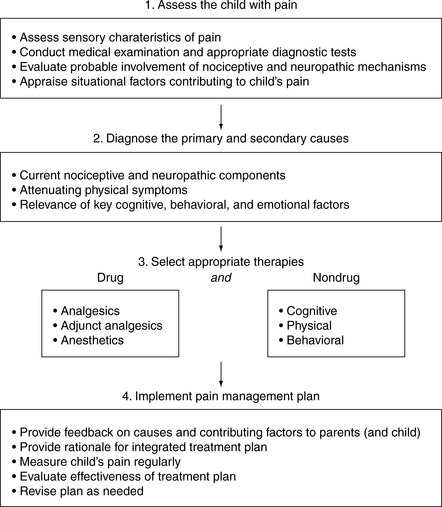
Figure 30-3 A treatment algorithm for controlling children’s pain.
(From McGrath PA, Brown SC: Pain control in paediatric palliative care. In Doyle D, Hanks GW, MacDonald N, editors: Oxford textbook of palliative medicine, 3rd ed, Oxford, in press, Oxford University Press, with permission.)




