PAIN: CHEST
ROBYN L. BYER, MD
The complaint of chest pain rarely represents a life-threatening emergency in children, in contrast to the same complaint in adults. Although heart disease is an uncommon source of chest pain in children, the fear of a cardiac origin for the pain may evoke anxiety in the child or in the parents. There are a wide variety of etiologies for chest pain including diseases of the respiratory, cardiac, gastrointestinal (GI), neurologic, psychiatric, and musculoskeletal systems; however, it is most commonly due to idiopathic noncardiac origins. Chest pain accounts for approximately 0.6% of all pediatric emergency room visits and affects boys and girls equally. Clinicians need to take a careful approach to the patient even in the pediatric setting. This chapter first briefly reviews the pathophysiology of chest pain, then outlines the differential diagnosis in children, and finally presents the evaluation, as appropriate in the emergency department (ED).
PATHOPHYSIOLOGY
To understand the possible origins of chest pain or discomfort, it is important to review how this sensation is transmitted. Musculoskeletal pain is produced by irritation of tissues and is transmitted through the sensory nerves. The stimulus is carried through the nerve in the dermatomal or intercostals distribution to the dorsal root ganglia, up the spinal afferents, and into the central nervous system (CNS). This local, peripheral sharp pain can also be produced by primary dorsal root irritation in the spine. Because of overlap of nerve distribution, pain may be sensed in locations distal to the irritation. For example, the third and fourth cervical nerves evoke pain as far caudally as the nipple line of the chest.
Tracheobronchial pain is transmitted by vagal afferents in the large bronchi and trachea to fibers in the cervical spinal column. Dull, aching, or sharp pain is felt in the anterior chest or neck. The irritation or sensation of cough is transmitted in a similar fashion. Pleural pain arises in the pain-sensitive parietal pleura and then travels through the intercostals nerves in the chest wall, giving rise to sharp, well-localized pain. The visceral pleura is insensitive to pain. The intercostal or phrenic nerves transmit diaphragmatic pain. Peripheral diaphragmatic irritation may cause local chest wall pain because of the intercostals innervation. Central diaphragmatic stimulation travels by the phrenic nerve, with the distribution of pain referred to the shoulder of the affected side.
The esophagus appears to be more pain sensitive in its proximal portion. Pain is transmitted by afferents to corresponding spinal segments, with resultant anterior chest or neck pain. The pericardium is innervated by portions of the phrenic, vagal, and recurrent laryngeal nerves, as well as by the esophageal plexus. This appears to give rise to various sensations, including chest or abdominal pain, dull pressure, and even referred angina-like pain.
Other mediastinal structures, such as the aorta, have pain fibers in the adventitia of the vessel wall. They transmit pain through the thoracic sympathetic chain to the spinal dorsal roots, giving rise to sharp, and variably localized chest pain. Cardiac pain probably is transmitted by a number of routes, including the thoracic sympathetic chain and the cardiac nerves through the cervical and stellate ganglia. It has been proposed that pain arises from abnormal ventricular wall movement and stimulation of the pericardial pain fibers. These routes account for the sensation of cardiac chest pain as pressure or crushing pain substernally or as sharp pain in the shoulder, neck, or arm.
DIFFERENTIAL DIAGNOSIS
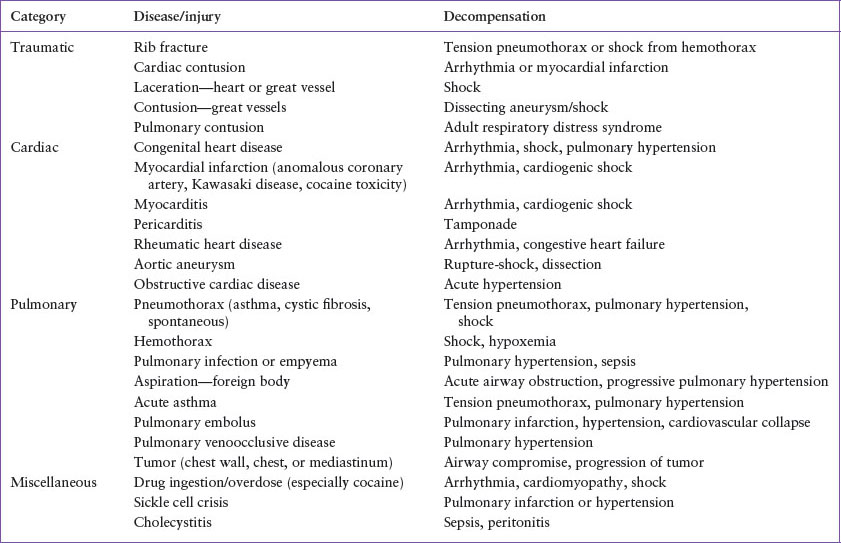
A differential diagnosis of chest pain in children is included in Table 50.1. In the case of trauma, cardiac or pulmonary compromise may arise from direct injury to the heart, great vessels, or lung (see Chapter 123 Thoracic Trauma). Most chest pain in the nontraumatized child is caused by acute respiratory disease, musculoskeletal injury, anxiety, or inflammation (Table 50.2). Often, the physician does not make a causative diagnosis of the chest pain and calls it nonspecific or idiopathic in origin. Occasionally, this idiopathic chest pain may be unrecognized organic disease, such as gastroesophageal reflux disease. Chest pain in children usually occurs without associated cardiorespiratory signs or symptoms, often as an acute or chronic problem. By the time of the ED visit, frequently the pain has resolved. Although much less frequent, chest pain in association with cardiorespiratory distress demands immediate attention. Table 50.3 lists the life-threatening causes of chest pain by disease and mechanisms for decompensation. Chest pain in the dyspneic or cyanotic patient most often stems from a respiratory problem, such as pneumonia, asthma, pleurisy, or pneumothorax. Rarely does severe chest pain in an acutely ill child result from myocardial infarction (MI) due to aberrant coronary vessels, cocaine abuse, Kawasaki disease, hyperlipidemia, or other underlying cardiac diseases (aortic stenosis, an acute arrhythmia, or pericardial disease). Every individual evaluation must be started, however, with a broad differential diagnosis in mind to ensure proper diagnosis and management of the child with chest pain.
Although studies range in estimating a cardiac cause for chest pain in a pediatric patient, it is generally very low, <6%. The largest most recent study of pediatric patients with chest pain in a pediatric emergency setting found a cardiac cause for chest pain to be 0.6%. Major categories include arrhythmias, anatomic lesions, and acquired disorders such as myocarditis and pericarditis. Myocardial ischemia is very rare in pediatrics but can present with typical unrelenting substernal crushing chest pain with or without radiation to neck or arm, diaphoresis, nausea, dyspnea, and syncope. Patients are usually in distress and have physical examination abnormalities including pallor, diaphoresis, a gallop rhythm, a heart murmur, and decreased peripheral perfusion. Myocardial ischemia/infarction can occur as a result of a thrombosed coronary artery aneurysm. These aneurysms, which occur as a sequelae from Kawasaki disease, have both insufficient laminar flow and areas of stenosis that become obstructed via thrombosis leading to decreased myocardial perfusion. Case reports of myocardial ischemia without risk factors in adolescents have been attributed to vasospasm. Cocaine exposure can result in palpitations and coronary vasospasm leading to ischemia, MI, arrhythmias, or cardiomyopathy. Patients with cocaine toxicity are often anxious with confusion or combativeness and have significant tachycardia and hypertension. Other toxins have cardiac effects. The herbal medications aconite, ephedra, and licorice have also been implicated as the cause of chest pain, congestive heart failure, arrhythmias, and MIs.
TABLE 50.1
CAUSES OF CHEST PAIN
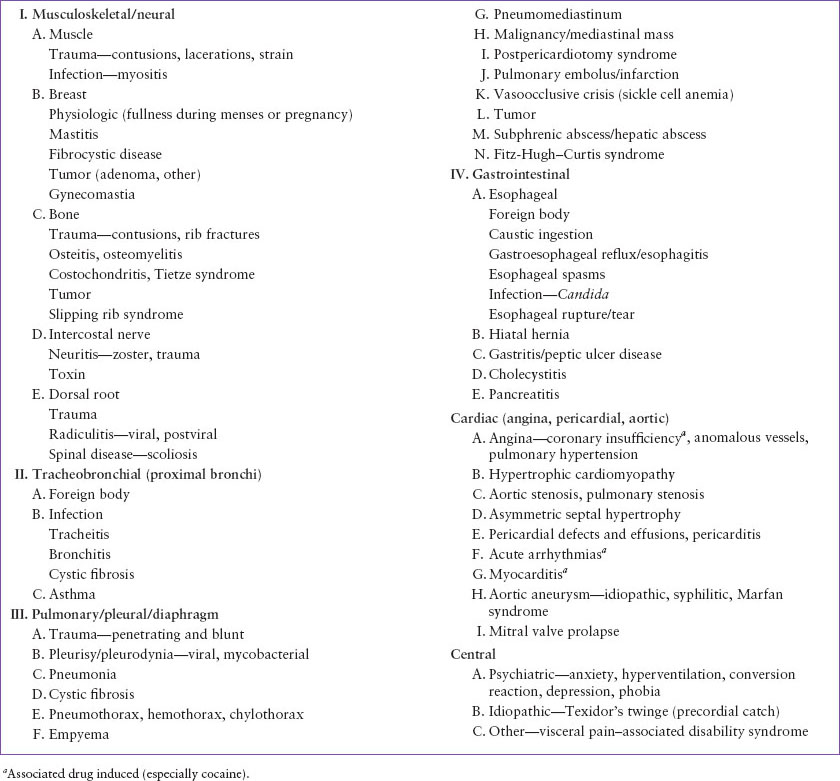
TABLE 50.2
COMMON CAUSES OF CHEST PAIN
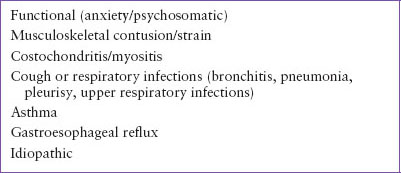
TABLE 50.3
LIFE-THREATENING CAUSES OF CHEST PAIN
Anomalous coronary arteries which originate from the opposite sinus and traverse between the great vessels usually present with sudden death but can also cause chest pain with intense exercise. Pain is thought to be related to inadequate coronary perfusion via either compression of the great vessels, relative ostial stenosis, or both. The history is the key to this significant disease as the physical examination is usually normal.
Hypertrophic cardiomyopathy is the most common cardiac cause of sudden death, which is likely due to ventricular dysrhythmias, yet chest pain is not a common feature. This disease follows an autosomal dominant pattern of inheritance; however, spontaneous mutations may occur. Patients often have a systolic murmur which becomes more intense with standing or a Valsalva maneuver. Chest pain can also occur with severe obstruction from aortic stenosis which is likely to be discovered by the pathologic murmur on physical examination. The patient with chest pain that has onset with or worsening with exertion should be evaluated for these conditions.
Arrhythmias are not uncommon and children usually present with palpitations or a combination of chest pain and palpitations. Symptoms of heart pounding may occur with instantaneous initiation and termination whereas other children have been reported to abruptly stop an activity. Most arrhythmias are benign, such as premature atrial and ventricular contractions; however, children may present with signs of shock, congestive heart failure, or syncope secondary to supraventricular or ventricular tachycardia. Physical examination is often normal in the absence of active arrhythmias but long-term effects can lead to cardiomyopathy. Dilated cardiomyopathy presents with chest discomfort, fatigue, exercise intolerance, palpitations, and physical examination findings such as a gallop rhythm and a murmur secondary to mitral valve insufficiency.
Inflammatory conditions such as pericarditis and myocarditis can present with chest pain and systemic symptoms. Pericardial disease includes pericarditis, pericardial effusions, and cardiac tamponade. Pericarditis often presents with fever, a stabbing chest pain that improves with sitting up and leaning forward, respiratory distress, a friction rub, and distant heart sounds. Pericarditis and pericardial effusions can restrict outflow leading to neck vein distention and in severe cases of tamponade, pulsus paradoxus (see Chapter 94 Cardiac Emergencies). The presentation of myocarditis can be more subtle with mild chest pain and fatigue for several days followed by the development of fever, dyspnea, and worsening chest pain. The examination often shows tachycardia (or bradycardia when severe), orthostatic changes not improved by fluid resuscitation, pulsus paradoxus, and a gallop rhythm. Both pericarditis and myocarditis are usually associated with a preceding viral illness. Endocarditis is most often seen in children with a history of congenital heart disease but can present in those with no known predisposing condition. Patients are often ill appearing with a history of prolonged fever and may have signs of embolization. Other illnesses that can present with carditis include rheumatic heart disease and Kawasaki disease.
Chest pain associated with mitral valve prolapse is controversial. Studies have shown that mitral valve prolapse is not more common in those with chest pain than in the general population and other etiologies of the chest pain may exist in a patient with this condition. However, chest pain in patients with mitral valve prolapse may be secondary to papillary muscle or left ventricular endocardial ischemia. A midsystolic click and late systolic murmur should be found on physical examination. Pain secondary to mitral valve prolapse should be considered only when no other etiology may be found.
Patients with connective tissue disorders such as Marfan syndrome have the potential to develop aortic dilation, aortic dissection, and rupture. Symptoms of aortic dissection/rupture include generalized distress with unrelenting severe chest pain, decreased cardiac output, dyspnea, and often abdominal pain.
Children who present with chest pain days to months after cardiac surgery should be evaluated for signs of pericardial effusion known as postpericardiotomy syndrome. Patients with pulmonary hypertension may present with exercise intolerance, palpitations, and syncope. The resultant right ventricular dilatation may be found on physical examination as a narrowed second heart sound, hepatomegaly, and cyanosis if an ASD or VSD is present. Eisenmenger syndrome is severe pulmonary hypertension from an uncorrected congenital heart disease leading to cyanosis from right-to-left shunting of blood. Isolated anatomic abnormalities such as atrial septal defects have been known to present with chest pain and may or may not display the classic findings of a hyperactive precordium, widely split fixed second heart sounds, and both a systolic and diastolic murmur.
Unrecognized disease rarely causes isolated chest pain in a child who otherwise appears well, but the physician should consider drug exposure (e.g., cocaine; methamphetamine; nicotine; beta-agonist abuse; the triptans; combination of cold medications containing chlorpheniramine, dextromethorphan, and phenylpropanolamine; and herbal medications mentioned previously). Although cardiac conditions are infrequent, attention should be paid to diagnosing the rare patient with hypertrophic cardiomyopathy, angina, mitral valve prolapse, or early pericardial or myocardial inflammation (see Chapter 94 Cardiac Emergencies).
Pulmonary diseases are common and account for approximately 12% to 21% of chest pain cases. A first episode of reactive airway disease should be suspected when an associated night cough, history of wheezing, or family history of atopy is present. There is a high incidence of exercise-induced asthma which often presents with chest tightness, shortness of breath, and wheezing with exercise. These historical features are important as the physical examination may be completely normal during the ER visit. Infectious diseases of the respiratory tract are associated with fever, malaise, cough, and coryza, and may involve several family members simultaneously. Patients with pneumonia (see Chapter 107 Pulmonary Emergencies) often present with tachypnea and hypoxia in addition to fever and cough. Spontaneous (nontraumatic) pneumomediastinum and pneumothorax may occur in patients with reactive airway disease, cystic fibrosis, or as a result of barotrauma (i.e., Valsalva maneuver, forceful vomiting, or coughing). The pain of a pneumothorax is often unrelenting and pleuritic in nature. If the pneumothorax is moderate or large, then patients present with significant respiratory distress and decreased breath sounds on the affected side. Spontaneous (nontraumatic) pneumomediastinum is most often reported in male adolescents without underlying lung disease and those with asthma. It appears to occur with any activity that involves straining against a closed glottis. This is thought to cause a rise in intra-alveolar pressure and subsequently a rupture of the alveoli releasing air into the interstitial space. Air then dissects along facial planes of the hilum into the mediastinum and neck. Those with spontaneous pneumomediastinu m present with substernal chest pain which frequently radiates to the neck and is worse with deep inspiration and position changes, subcutaneous crepitus, Hamman sign (crunching heart sounds), dysphagia, and dysphonia. This diagnosis must be distinguished from pneumothorax, pericarditis, and esophageal perforation.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


