Key Clinical Questions
Osteomyelitis: Introduction
Osteomyelitis is bone infection with accompanying inflammation and bone destruction. Bone resists infection under normal circumstances. Factors that influence the establishment and progression of osteomyelitis include the virulence of the pathogen, inoculum size, characteristics of the involved bone, presence of foreign objects, host immune system, and duration of infection. Bone may be infected by direct contamination during trauma or surgery, spread of infection from adjacent soft tissue, or hematogenous seeding of microbes. The diagnostic and therapeutic approach varies depending on the mode of infection. However, as treatment for osteomyelitis is long, complex, expensive, and not always successful even when management is optimal, proper diagnosis and pathogen identification is of great importance in all cases.
Pathophysiology
Bacteria infect bone through trauma or surgery, spread from adjacent soft tissue, or bacteremic seeding. They then attach to host cells and extracellular matrix components, as well as implanted biomaterials, if present. Bacterial strategies to evade the host immune response include elaboration of biofilm, a hydrated matrix that establishes a physical barrier against both host defenses and antibiotics. Bacteria embedded in biofilm are also less metabolically active, making them less susceptible to antibiotics. Inflammation associated with bacterial toxins and the host immune response leads to bone lysis. Over time, as infection becomes chronic, suppuration leads to vascular congestion, raised intraosseous pressure, and ischemia of infected bone. The necrotic bone separates from healthy bone to form a sequestrum, a diagnostic finding of chronic osteomyelitis. If the dead bone cannot be resorbed, new bone may form from the surrounding healthy bone tissue, encasing the sequestrum in an involucrum. The walled-off sequestrum may become functionally similar to an abscess, with bacterial growth continuing in a pocket of necrotic tissue inaccessible to immune surveillance or antibiotics. As pressure in the sequestrum builds, infection may erupt through the involucrum, leading to subperiosteal or soft tissue abscesses, or a sinus tract through overlying soft tissue.
|
Does This Patient Have Osteomyelitis?
The evaluation for osteomyelitis begins with the history and physical exam. Patients should be asked about risk factors for osteomyelitis, such as diabetes, vascular disease, intravenous drug use, and recent trauma or surgery. Physical findings of osteomyelitis may include sinus tracts, nonhealing wounds and ulcers that probe to bone, and evidence of associated peripheral vascular disease or diabetes. However, the exam is often unrevealing, especially in hematogenous osteomyelitis of deep sites. Laboratory evaluation includes blood cultures, white blood cell (WBC) count with differential, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) level. The WBC count is usually nonspecific and more often elevated in acute than chronic osteomyelitis. ESR and CRP can be elevated in many conditions and may also be normal early in osteomyelitis. If ESR and CRP are elevated due to osteomyelitis, they can be used to assess patient response to treatment. CRP may drop within one to two weeks of starting appropriate therapy, while ESR falls more slowly. Other serum markers associated with bone disease, such as calcium, phosphate, and alkaline phosphatase, are usually normal in osteomyelitis.
The initial radiographic study in suspected osteomyelitis should be plain films of the affected area. These may show soft-tissue swelling, narrowing or widening of joint spaces, bone destruction, and periosteal reaction. If plain radiographs suggest osteomyelitis and blood cultures are positive, a presumptive diagnosis can be made and no further evaluation is needed. When plain films are not diagnostic, MRI should be the next radiologic study to diagnose osteomyelitis. MRI and CT are both useful in revealing medullary and cortical destruction, periosteal reaction, articular damage, and soft-tissue involvement. MRI is better for diagnosing soft tissue involvement, and CT is more sensitive for detecting cortical and medullary sequestra. Overall, MRI is more sensitive than CT, and also does not expose the patient to radiation. Bone marrow edema on MRI may be seen as early as three days into the course of osteomyelitis. However, MRI is not helpful in assessing the response to therapy, as bone marrow edema persists for months after microbiological cure. Another limitation is that bone marrow edema on MRI is not specific for osteomyelitis: it may also be caused by trauma, Charcot arthropathy, and surgery. Radionuclide bone scans have similar sensitivity to MRI, but also similar problems with specificity, as well as much lower spatial resolution. They may be useful in the presence of orthopedic devices which create artifacts on CT and MRI.
Isolation of a microbial pathogen via bone biopsy, along with histologic findings of inflammation and osteonecrosis, is the gold standard for the diagnosis of osteomyelitis. Antibiotics should be held before biopsy to maximize the yield of cultures, unless the patient is prohibitively ill. Percutaneous bone sampling should be pursued when feasible, but is limited by sampling error. Larger needles increase the diagnostic yield. The biopsy should be performed through healthy tissue under direct imaging guidance. If percutaneous biopsy and blood cultures are negative, and clinical suspicion of osteomyelitis remains high, then percutaneous biopsy should be repeated, or an open biopsy performed. Open bone biopsy provides the best results, but is more morbid. In patients with overlying wounds or sinus tracts, microbes cultured from superficial samples are often nonpathogenic, and correlate poorly with those responsible for the deep osteomyelitic infection, with the significant exception that identification of Staphylococcus aureus usually correlates with deep infection.
Osteomyelitis from Direct Inoculation
Direct inoculation of bone tissue by pathogens may take place during surgery or orthopedic trauma. The risk of osteomyelitis after an open fracture depends on the type of fracture, degree of contamination, surrounding soft tissue injury, and timing of local or systemic antibiotics after contamination. Commonly involved organisms include staphylococci, gram-negative bacilli, and other skin flora and soil organisms. As these patients often undergo multiple surgical procedures, they are also at risk for nosocomial pathogens.
Acute trauma–associated osteomyelitis can often go undiagnosed, as the initial signs can be mistaken for inflammation from other causes associated with the episode of trauma. As untreated acute osteomyelitis progresses to chronic osteomyelitis, signs and symptoms indicative of chronic osteomyelitis, such as fracture nonunion, poor wound healing, and sinus tract formation, may appear. Plain radiographs are often unhelpful, as traumatic and postoperative changes confound interpretation. MRI is sensitive, but less specific in this setting. It is reasonable to pursue another imaging modality, such as CT or radionuclide bone scan, prior to surgical intervention.
The management principles for open fracture include early treatment with surgical debridement and administration of a short course of antimicrobial prophylaxis to prevent osteomyelitis. When osteomyelitis develops, the practice principles are microbe identification, surgical debridement, and tailored antibiotic therapy. The presence of foreign objects, such as fixation devices, requires long term oral antimicrobial therapy until fracture healing and removal of the fixation devices. When oral suppression fails to result in fracture healing, definitive therapy with removal of foreign objects, further surgical debridement, and additional directed antimicrobial therapy should be considered.
Osteomyelitis from Adjacent Soft Tissue Infection
Individuals with diabetes and peripheral vascular disease are the population at highest risk from this type of osteomyelitis, especially in the foot. Peripheral neuropathy predisposes to soft tissue ulceration in the feet, and vascular disease impairs proper immune response and wound healing. A significant percentage of these patients ultimately require amputation due to chronic soft tissue and bone infections.
Patients may have no fever and few signs of inflammation. The persistence of soft tissue inflammation and ulceration for a week or longer, however, should raise suspicion for underlying osteomyelitis. Physical exam should include the evaluation of pulses and Doppler ultrasound measurement of vascular flow, as well as characterization of neuropathy. If necessary, a more detailed evaluation including arteriography and nerve conduction studies could be considered.
One of the most useful tests for osteomyelitis in patients with soft tissue wounds is the “probe-to-bone” test, which involves advancing a sterile surgical probe through the ulceration. If the probe reaches bone, then the bone is almost certainly infected. In patients with diabetic foot ulcers, an ulcer that measures more than 2 cm2 is strongly suggestive of osteomyelitis (Table 200-1). If suspicion remains high in the absence of convincing data from clinical exam and plain films, MRI is a sensitive and specific tool to assist in confirming infection.
| Risk Factors/Findings | Positive LR | Negative LR |
|---|---|---|
| Probe to bone | 6.4 | 0.39 |
| Bone exposure | 9.2 | 0.70 |
| Ulcer area > 2 cm | 7.2 | 0.48 |
| Ulcer inflammation | 1.5 | 0.84 |
| Clinical gestalt | 5.5 | 0.54 |
| Erythrocyte sedimentate rate > 70 | 11 | 0.34 |
These infections are frequently polymicrobial, and include aerobic and anaerobic gram-positive and negative bacteria, with staphylococcal and streptococcal species commonly involved. Treatment usually requires a combination of broad spectrum antimicrobial treatment and surgical intervention, such as debridement or amputation. Often, revascularization is a critical part of the treatment plan, as debridement and antibiotics will fail to clear an infection unless the vascular supply is adequate. The duration of antimicrobial treatment should be at least six weeks. Some argue that antimicrobial therapy should continue until complete resolution of the skin and soft tissue defects.
Hematogenous Osteomyelitis
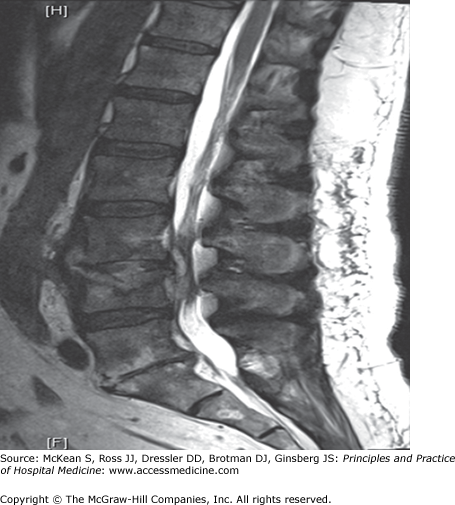
Any bone can be seeded by hematogenous spread of microbes, but in adults the spine is most often affected. Vertebral osteomyelitis, or spondylodiscitis, commonly involves the lower thoracic or lumbar spine and less frequently the cervical spine, often presenting as lower back pain or torticollis, respectively. Vertebrae are well perfused, and neighboring vertebrae share segmental arteries. Infection therefore often involves adjacent vertebrae with their intervertebral disc (Figure 200-1). Epidural or psoas abscesses are common complications. The source of bacteremia may include skin and soft tissue infections, urinary tract infections, dental abscesses, and central venous catheter–associated infections, but it is often unidentified.
Related posts:
 Strategies for Cost-Effective Care
Strategies for Cost-Effective Care
 Building, Growing, and Managing a Hospitalist Practice
Building, Growing, and Managing a Hospitalist Practice
 Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
 Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist
Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


