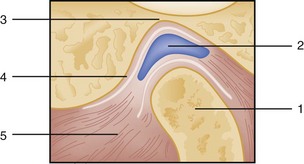
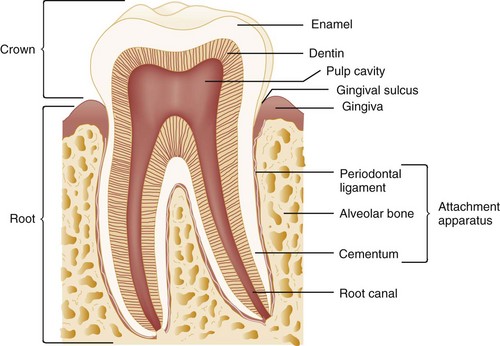
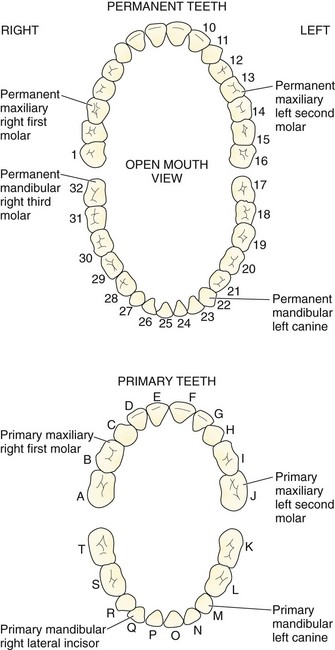
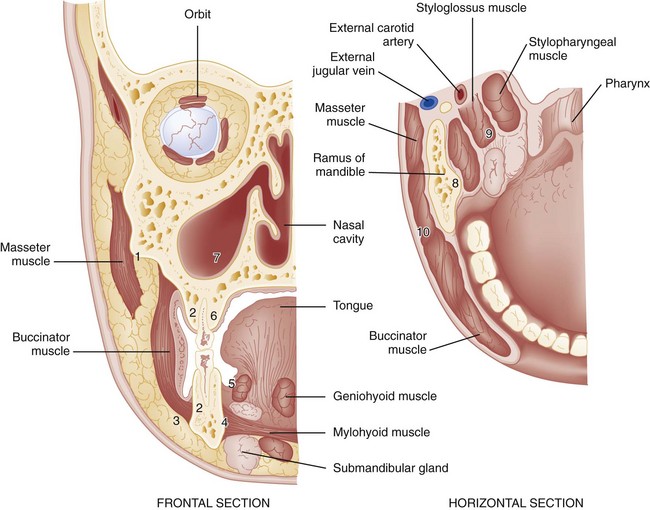
Chapter 70 The mandible is formed by two rami that divide into a horizontal and an ascending portion. The horizontal portion forms the body of the mandible. The ascending ramus divides into the coronoid process anteriorly and the condylar process posteriorly. The temporomandibular articulation is unique because it consists of a bilateral joint, or diarthrosis, between the mandibular fossa and articular eminence of the mandible’s temporal bone and condyle (Fig. 70-1). An intervening layer of fibrous connective tissue separates the articulating surfaces. A fibrous capsule also surrounds the temporomandibular joint (TMJ) and is reinforced by capsular ligaments that help limit mandibular range of motion. Functionally, when the mandible opens, the condyles move inferiorly and anteriorly down the eminence; during closure, the mandible moves posteriorly along the eminence and superiorly into the fossa. The pulp is the tooth’s center and serves as its neurovascular supply. The primary purpose of the pulp is to provide sensation and to produce dentin, a microtubular structure that hydrates and cushions the tooth during mastication. The part of the tooth normally visible in the oral cavity is the coronal portion covered with enamel, the hardest substance in the body. The part that is not normally visible and anchors the tooth is called the root. The root is covered with cementum, which is much softer than enamel and not designed for exposure in the oral cavity (Fig. 70-2). The normal primary, or deciduous, dentition consists of 10 mandibular and 10 maxillary teeth. The primary dentition is important for mastication, cosmesis, and growth and development and functions as a physiologic space maintainer. Starting at the midline and moving posteriorly in any quadrant, the normal dentition consists of a central incisor, lateral incisor, canine, and two primary molars. The lower central incisor is the first tooth to erupt, at approximately 6 months of age; all primary teeth should be present by 3 years of age. If not, further investigation for developmental or endocrine abnormalities is warranted. The permanent dentition begins to erupt at approximately 5 to 6 years of age with the appearance of the first molar. Normally, the permanent dentition consists of 32 teeth: the central incisor, lateral incisor, canine, two premolars, and three molars. The third molars are the last to erupt, appearing at approximately 16 to 18 years of age, and are commonly called “wisdom teeth.” The primary molars are replaced by the permanent premolars. There are many numbering systems for teeth, but none are universal. Perhaps the most common system for the permanent dentition consists of numbering the teeth from 1 to 32, starting with the upper right third molar (1) and moving to the upper left third molar (16), to the lower left third molar (17), and to the lower right third molar (32). The starting point for this numbering system can be recalled by the mnemonic “upright.” Because there may be congenital absence of teeth or additional, supernumerary teeth, it is perhaps best for practitioners to describe anatomically which tooth is involved—for example, the upper left second premolar or the lower right second molar (Fig. 70-3). The periodontium consists of the gingival unit and the attachment apparatus. The gingiva is covered with keratinized, stratified, squamous epithelium and invests the tooth and alveolar bone. Apical to the gingiva is the alveolar mucosa, which is covered by nonkeratinized epithelium and is more subject to trauma. In healthy individuals the gingiva is attached firmly to the tooth by connective tissue fibers inserting into the cementum, extending coronally from the alveolar bone to the cementoenamel junction. A 2- to 3-mm cuff of tissue, the gingival sulcus, is bordered by the enamel surface of the tooth, the gingival epithelium, and the junctional epithelium at its base (see Fig. 70-2). In a disease state, such as in the presence of the loss of alveolar bone, this cuff increases in depth and is called a “pocket.” The fascial planes of the head and neck are defined as potential spaces filled with loose areolar tissue that separates the layers of fascia of the head and neck. The deep cervical fascia is most important in a discussion of the extension of oral infection to the head and neck (Fig. 70-4). The deep cervical fascia consists of the superficial and investing layer, the pretracheal layer, the prevertebral layer, and the carotid sheath. The superficial and investing layer surrounds the entire neck; it splits as it attaches to the inferior border of the internal pterygoid muscles at the mandible’s ascending ramus. This split forms the masticator space. This space communicates superiorly above the level of the zygomatic arch with the superficial and deep temporal pouches. Nontraumatic Dental Emergencies Two pathophysiologic processes affect the dental health of most of the population: (1) dental caries and (2) periodontal disease. Variables related to both disease states include the oral environment, consisting of the teeth and attachment apparatus; the presence of local factors such as bacterial plaque, oral microflora, and substrate; and host states, including immunocompromising diseases and nutritional status. Factors such as water fluoridation, fluoride supplements, and plaque control techniques (e.g., flossing, brushing, orthodontic and dental surgical procedures) have significantly decreased the prevalence of dental caries and periodontal disease. However, the emergency department (ED) is the frequent source of care for dental emergencies, with toothache related to dental caries being the most common complaint. This occurs because of both lack of after-hours access for dental complaints and socioeconomic factors (self-pay and Medicaid). A recent study from Kansas City shows an increased volume from 2001 to 2006 from 13.1% up to 19%.1 Pus leaks from the apex of the root and forms an abscess; this is termed a periapical abscess. Periapical abscesses are confined within the alveolar bone (Fig. 70-5). The abscess may break through the cortical plate of either the mandible or the maxilla and spread subperiosteally. Subperiosteal extensions are generally well confined anatomically by muscle attachments; however, if the muscle attachments are violated, either during a surgical procedure or by the natural extension of an infective process, the bacteria can gain access to the fascial planes of the head and neck. Infection extending to the submaxillary, sublingual, and submental spaces with elevation of the tongue is called Ludwig‘s angina. Ludwig’s angina is one of the most serious mandibular infections because of its potential for airway obstruction. Examination of the Oral Cavity The examiner should wear eye protection, a mask, and gloves in compliance with universal precautions when examining the oral cavity. Ideally the patient should be placed in a dental or ear, nose, and throat chair or on a cart at a 45-degree angle. Because pediatric patients are unlikely to cooperate with the examination, the following technique is used by some experienced practitioners. The child sits in the parent’s lap, or the child is first placed in the parent’s lap facing the parent. The examiner then sits in front of the parent. While the parent gently restrains the child’s arms and legs, the emergency physician can lean the child backward and lock the child’s head between the physician’s legs.2 Radiographic evaluation of teeth is best accomplished with dental (periapical) films. These films are generally not available in the ED, however. A panoramic radiograph is a useful alternative (see Fig. 70-5). Radiographic evaluation of teeth is ideally accomplished using dental (periapical) films, but these films are generally not available in the ED. More commonly, the panoramic radiograph is a useful alternative if imaging is felt to be required (see Fig. 70-5). The diagnosis and treatment of a dental abscess, for example, can be determined on the basis of clinical examination alone. A recent study compared the use of ED bedside ultrasound with the use of a panoramic radiograph. The sensitivity and specificity of the ultrasound were 92% and 100%, respectively. The advantage of the ultrasound is the lack of ionizing radiation; in addition, it assists in the determination of the presence of pus for incision and drainage.3 Computed tomography (CT) is used primarily when there is concern for deep space abscesses. Palliative management is indicated for most odontalgia. Systemic analgesics, such as nonsteroidal anti-inflammatory drugs (NSAIDs) or synthetic opioid agents, are indicated. In a meta-analysis of 11 studies comparing flurbiprofen, 65 to 70% of patients experienced 50% pain relief compared with 25 to 30% with placebo; this was similar to findings with comparable NSAIDs, and patients had similar need for rescue pain control at 6 hours.4 Although NSAIDs should be sufficient for most pain resulting from carious teeth, a therapeutic dental block may offer immediate relief. Synthetic opioids also are useful and are indicated in some cases but are generally not recommended in chronically carious teeth without an acute process.5 A limited quantity of analgesics should be dispensed, which encourages follow-up with a general dentist. Standard practice for years included starting the patient on phenoxymethylpenicillin (penicillin V) 250 mg four times daily or doxycycline 100 mg bid for 10 days and warm saline rinses and referring him or her to an oral maxillofacial surgeon or general dentist. Drains are removed in 24 to 48 hours, and antibiotics are continued for 7 to 10 days.5 However, recent reviews have questioned the need for routine prescribing of antibiotics if sufficient drainage of pus has been achieved.6,7 The presence of cellulitis or swelling in the contiguous spaces of the head and neck indicates the spread of a localized infection. In the early stages of such an infection, the upper half of the face is generally involved, with extension of infection from maxillary teeth; cellulitis from mandibular teeth generally involves extension to the lower half of the face and the neck (Fig. 70-6). More advanced infections may extend into any of the fascial planes of the head and neck down to the mediastinum. In the nondebilitated host, untreated dental infections tend to localize and drain spontaneously and extraorally. In the presence of a compromised host or aggressive microorganisms, spread into the fascial planes is more common, with a potential for greater morbidity and mortality. General indications for admission include suggested spread of infection to fascial planes, high fever, toxic appearance, trismus, and an immunocompromised host. The potential sequelae of sepsis and airway obstruction must be appreciated. CT of the head and neck can be useful if the diagnosis is in doubt. Airway management should be undertaken when indicated, particularly if signs or symptoms of impending airway obstruction are present or developing (altered voice, drooling, stridor). The intubation should be approached as a difficult airway, as outlined in Chapter 1. An ear, nose, and throat specialist or oral maxillofacial surgeon should be consulted for ongoing management, including determination of the site of the initial focus so that pus can be evacuated. Fever is common as with any infection. Any irritation of the internal pterygoid or masseter muscles results in trismus. Trismus is the inability to open the mouth because of involuntary muscle spasm. Trismus limits visualization of the pharynx and may make diagnosis of lateral or retropharyngeal space involvement difficult. Trismus is muscular in origin, not a result of impaired or augmented neuromuscular transmission, and so is often minimally improved or not improved at all after administration of a neuromuscular blocking agent (e.g., succinylcholine) for intubation, especially if the trismus is caused by localized swelling (vs. pain and spasm). Intubation in all patients with trismus is presumed to be difficult. Preparations should be made to perform a fiberoptic intubation or to establish a surgical airway.8 Difficulty swallowing or handling secretions suggests the possibility of retropharyngeal or parapharyngeal infection. Respiratory distress may be apparent, or the airway may occlude rapidly after a period of minimal signs of impending obstruction. Spread of mandibular dental infection frequently results in a cellulitis called Ludwig’s angina, a bilateral, boardlike swelling involving the submandibular, submental, and sublingual spaces with elevation of the tongue. The most serious immediate sequela is airway obstruction. A characteristic brawny induration is present; there is no fluctuance for incision and drainage. Hemolytic Streptococcus is most commonly responsible for the infection, although a mixed staphylococcal-streptococcal flora is common, and both may lead to an overgrowth of anaerobic gas-producing organisms, including Bacteroides fragilis. Treatment consists of antibiotics and airway management. Although oral intubation can be attempted, an “awake” technique is recommended (see Chapter 1) because inability to displace the tongue into the submandibular space with a laryngoscope may make oral intubation impossible; fiberoptic nasopharyngoscopy is an option progressing to cricothyrotomy. In a study of 10 cases of Ludwig’s angina requiring surgical decompression, after inhalational anesthesia, the vocal cords were visualized in 9 of the 10 patients. One patient required tracheostomy.
Oral Medicine
Perspective and Principles of Disease
Musculoskeletal Unit
Teeth
Periodontium
Fascial Planes of the Head and Neck
Pathophysiology
Clinical Features
Diagnostic Imaging
Dental Caries
Treatment
Simple Dental Abscess
Treatment
Spread of Infection to the Head and Neck
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Anesthesia Key
Fastest Anesthesia & Intensive Care & Emergency Medicine Insight Engine