Figure 36.1
Subcostal incision (dotted line) and vertical upper midline incision (solid line)
For oncological resections, careful inspection and palpation of the liver and peritoneal surfaces is performed to identify occult metastases that may potentially alter operative conduct. In selected cases, diagnostic laparoscopy may be useful in this regard (Fig. 36.2).
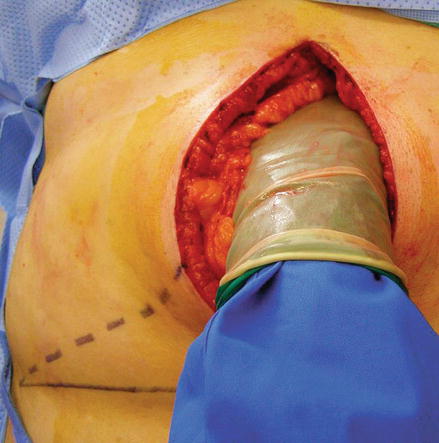
Figure 36.2
The abdomen is carefully explored
Exposure
The ligamentum teres is ligated and divided, and its proximal aspect can be used as a handle with which to elevate the left hemiliver (Fig. 36.3).
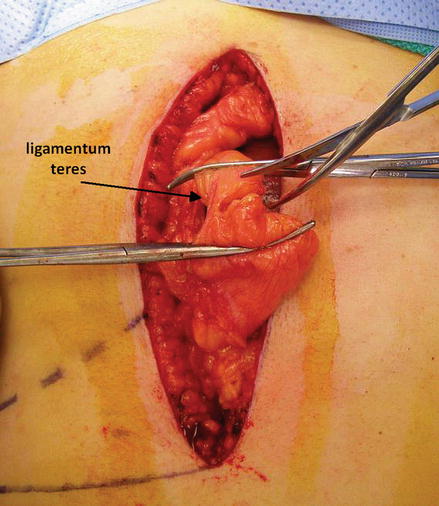
Figure 36.3
The ligamentum teres is ligated and divided
The falciform ligament is divided close to the liver from the ligamentum teres toward the confluence of the hepatic veins, and retractors are positioned to provide exposure of the liver (Fig. 36.4).
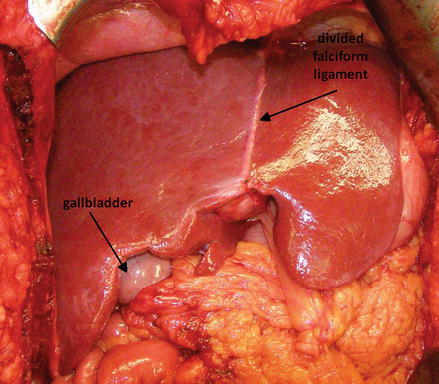
Figure 36.4
The falciform ligament is divided close to the liver from the ligamentum teres toward the confluence of the hepatic veins
Intraoperative hepatic ultrasonography is performed for evaluation of hepatic anatomy, tumor localization, and to exclude previously unidentified pathology (Fig. 36.5).

Figure 36.5
Intraoperative hepatic ultrasonogrphy
Right Hemihepatectomy (Segmentectomy V-VIII)
Exposure
The retroperitoneal attachments of the right hemiliver are incised, permitting elevation and medial rotation of the right hemiliver off the inferior vena cava and right adrenal gland. Here, the right triangular ligament is being incised (Fig. 36.6).
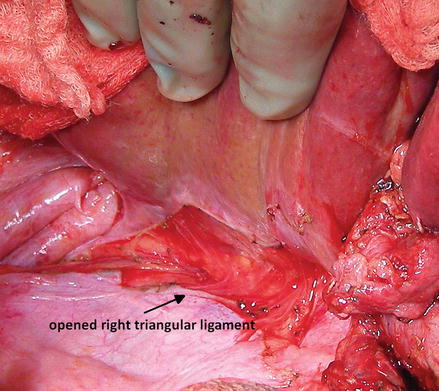
Figure 36.6
The right triangular ligament being incised
Inflow Control
The peritoneum overlying the porta hepatis is incised (Fig. 36.7).
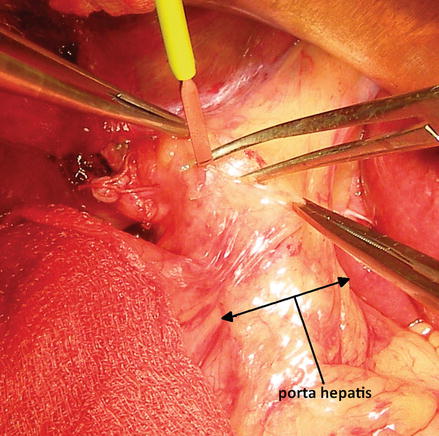
Figure 36.7
The peritoneum overlying the porta hepatis being incised
The right hepatic artery is identified, ligated, and divided (Figs. 36.8 and 36.9).
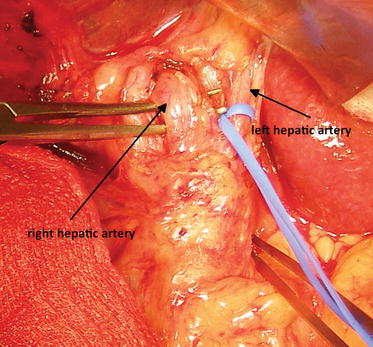
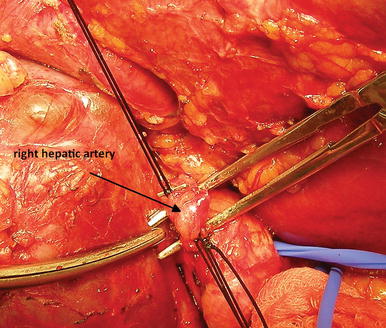
Figure 36.8
The right hepatic artery is identified, ligated, and divided (view 1)
Figure 36.9
The right hepatic artery is identified, ligated, and divided (view 2)
Division of the right hepatic artery facilitates exposure of the right portal vein, which is ligated and divided (Figs. 36.10 and 36.11).
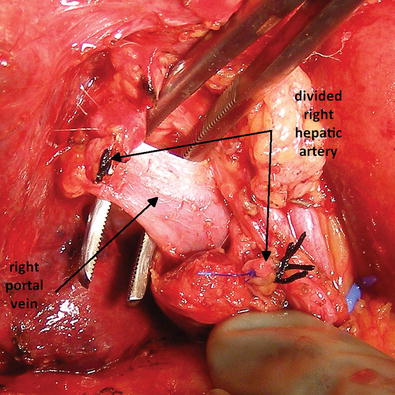
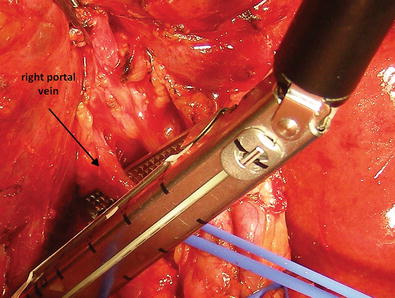
Figure 36.10
Division of the right hepatic artery
Figure 36.11
The right portal vein is ligated and divided
Division of the right hepatic inflow results in ischemic demarcation of the right hemiliver. The line of planned parenchymal transection is marked with electrocautery (Fig. 36.12).
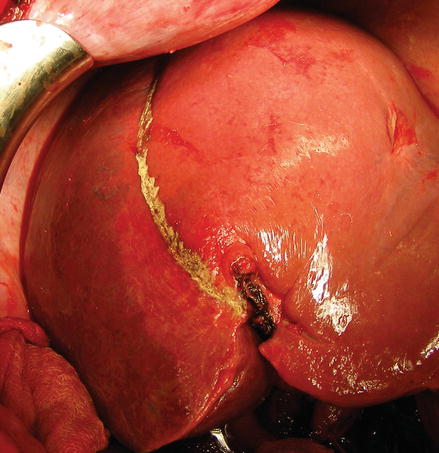
Figure 36.12
The line of planned parenchymal transection is marked with electrocautery
Outflow Control
Multiple draining veins between the right hemiliver and inferior vena cava are individually ligated and divided (Fig. 36.13).
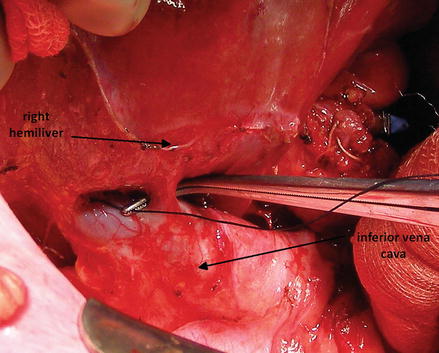
Figure 36.13
Multiple draining veins between the right hemiliver and inferior vena cava are individually ligated and divided
Dissection along the confluence of the hepatic veins permits identification of the junction between the right and middle hepatic veins. The right hepatic vein is encircled and transected (Figs. 36.14, 36.15, and 36.16).
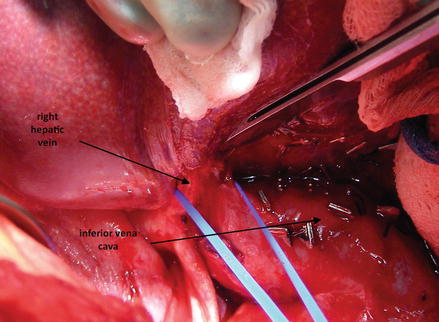
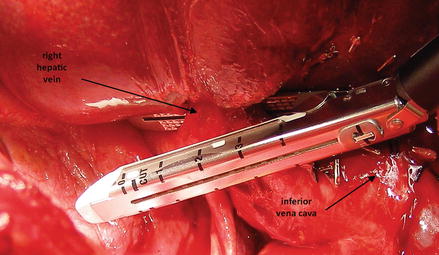
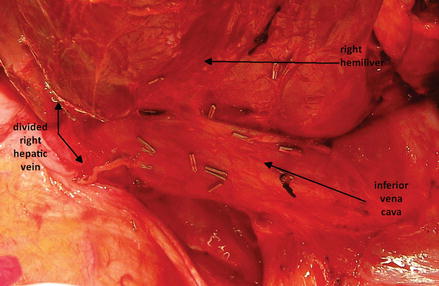
Figure 36.14
The right hepatic vein is encircled
Figure 36.15
The right hepatic vein is transected
Figure 36.16
The retrohepatic inferior vena cava is exposed
Parenchymal Transection
A Pringle maneuver may be performed by intermittently occluding the porta hepatis (Fig. 36.17).
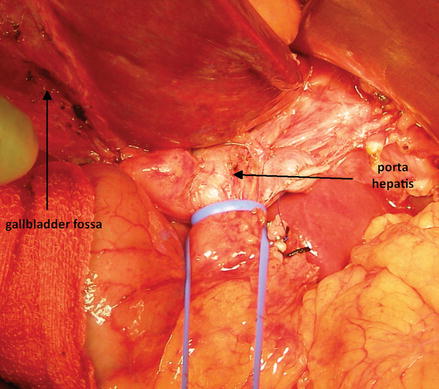
Figure 36.17
Pringle maneuver
Stay sutures placed along either side of the planned parenchymal transaction plane permit elevation and separation of the right and left hemilivers, facilitating exposure (Fig. 36.18).
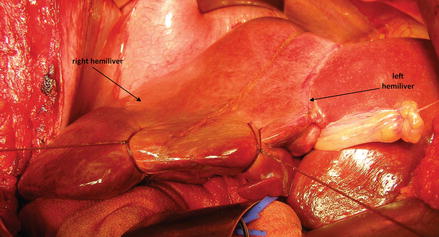
Figure 36.18
Stay sutures facilitate exposure of right and left hemilivers
Glisson’s capsule can be divided sharply; alternatively, parenchymal transaction can also be initiated using the harmonic scalpel (Figs. 36.19, 36.20, and 36.21).
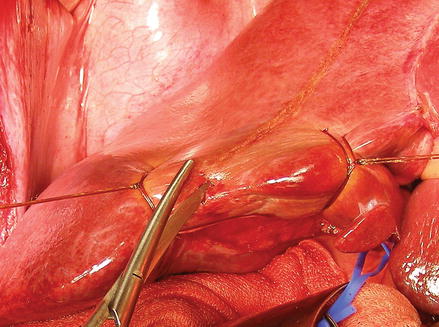


Figure 36.19
Glisson’s capsule being divided sharply
Figure 36.20
Parenchymal transaction initiated using the harmonic scalpel (view 1)
Figure 36.21
Parenchymal transaction initiated using the harmonic scalpel (view 2)
Crushing the hepatic parenchyma with a clamp permits visualization of biliary and vascular structures, which are individually ligated and divided (Figs. 36.22, 36.23, and 36.24).
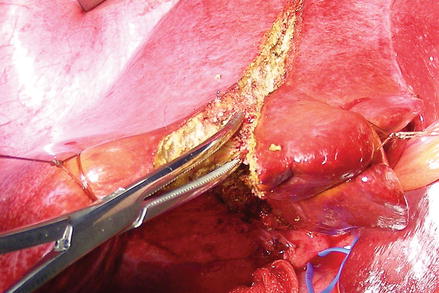
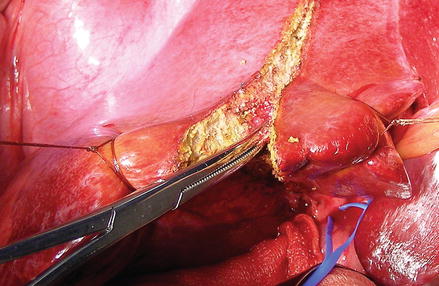
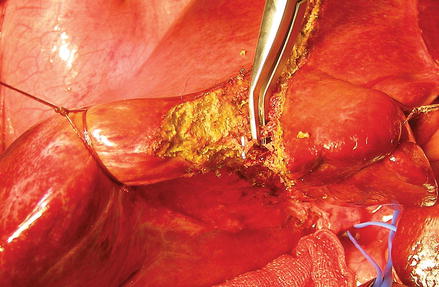
Figure 36.22
Crushing the hepatic parenchyma with a clamp permits visualization of biliary and vascular structures
Figure 36.23
Biliary and vascular structures are individually ligated and divided (view 1)
Figure 36.24
Biliary and vascular structures are individually ligated and divided (view 2)
Larger structures such as the middle hepatic vein may be divided with a stapler (Figs. 36.25 and 36.26).
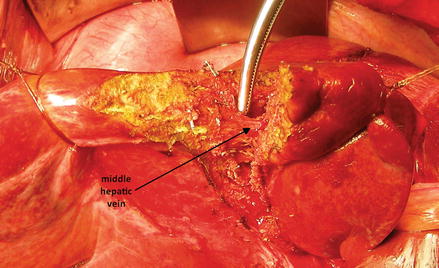
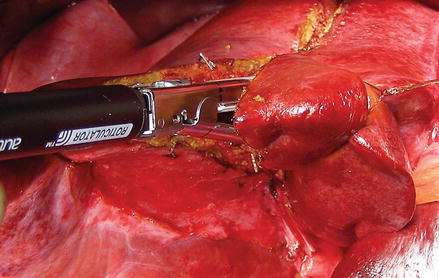
Figure 36.25
The middle hepatic vein divided with a stapler (view 1)
Figure 36.26
The middle hepatic vein divided with a stapler (view 2)
The specimen is removed, the cut surface of the liver is inspected to insure hemostasis and absence of bile leakage, and the abdomen is closed.
Left Hemihepatectomy (Segmentectomy II, III, IV)
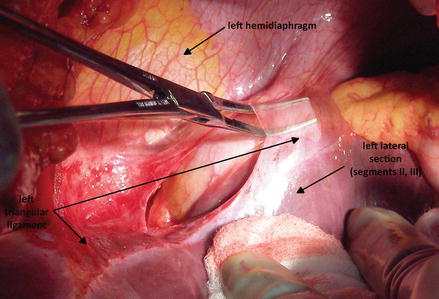
Exposure
The diaphragmatic attachments of the left hemiliver (the left triangular ligament) are divided, permitting medial rotation of the left lateral section of the liver (Fig. 36.27).