TOPICS
1. Minimally invasive surgical approaches
2. Anesthetic challenges for off-pump and minimally invasive surgery
3. Is off-pump surgery better than on-pump surgery?
During the 1990s the increased use of angioplasty and the development of stents for the treatment of coronary artery disease started surgeons on a quest to identify new, less invasive methods of treating heart disease. Surgeons attempted to perform coronary artery bypass through keyhole-sized incisions assisted by thoracoscopic techniques.1,2 Other surgeons attempted to use robotic surgery to reduce surgical incision size. Many more surgeons simply attributed most of the difficulties associated with cardiac surgery to the use of cardiopulmonary bypass (CPB). As such, they continued to operate on patients using a full sternotomy but completed their bypass grafts without the use of CPB—in essence operating on the beating heart.
All of these surgical innovations presented challenges for anesthesiologists at one time or another. During surgery with CPB the surgical manipulations of the heart do not generally affect the patient’s hemodynamics—after all the patient is on bypass. In the course of off-pump procedures, the heart must continue to beat and to supply blood to the tissues even when lifted out of the chest and potentially rendered ischemic during the sewing of vascular anastomoses. Consequently, the off-pump patient can deteriorate acutely requiring resuscitative measures and institution of emergency CPB. Never should off-pump cases be considered easy.
MINIMALLY INVASIVE SURGICAL APPROACHES
There are numerous surgical approaches that are designated as being “minimally invasive.” Many so called minimally invasive off-pump procedures are done through a fully invasive median sternotomy. So, minimally invasive and off pump are not necessarily the same thing. A surgeon can perform a minimally invasive procedure on bypass or a procedure can be performed without using bypass but through a full sternotomy.
For this discussion, minimally invasive implies that the surgeon is using something other than a full sternotomy to access the heart. The heart can be approached using various ministernotomies, thoracotomies, robotic ports, and/or thoracoscopic assistance. Many of these minimally access approaches will present different challenges to the anesthesiologist compared with the “routine” cardiac anesthesia described in Chapter 4.
Off-pump revascularization of the coronary arteries can be done through minimally invasive approaches or through a full sternotomy. When a full sternotomy is used as in off-pump coronary artery bypass surgery (OPCAB), the heart is lifted and manipulated using various support devices to permit the completion of multiple coronary bypass grafts. For the minimally invasive approach, a small thoracotomy is used and only the left internal mammary artery is generally grafted to the left anterior descending artery as in the minimally invasive direct coronary artery bypass (MIDCAB) technique. In either approach during “off-pump” bypass surgery the surgeon will occlude blood flow to the vessel being bypassed both proximally and distally using silastic snares and other occlusive devices. The surgical field is occasionally flooded with carbon dioxide to minimize entrainment of air into the coronary artery during surgical manipulation. Since the beating heart, when operated upon, presents the surgeon with a moving target there are various stabilization devices (Figure 13–1) commercially available, which relatively immobilize that region of the myocardium where the surgeon plans to create the bypass anastomoses. The surgeon must position the heart in such a manner that their access is suitable to complete the surgical repair. During positioning of the heart, venous return can be impaired leading to hemodynamic instability and hypotension. Often, however, once the heart is positioned in such a way that the graft can be placed, venous return becomes adequate and the heart pumps a suitable cardiac output to maintain the blood pressure even when lifted and retracted in the thorax. Frequently, the surgeon occludes the coronary artery to be bypassed for a brief period to determine the patient’s response to vessel occlusion and to possibly provide ischemic preconditioning. Following this trial the surgeon reperfuses the vessel in the hope that through ischemia preconditioning the myocardium supplied by that vessel will be more resilient to ischemia. The vessel is reoccluded and the anastomosis completed. During this period, the coronary artery being bypassed is ligated, and, thus, the myocardium dependent on that vessel’s flow distribution may become ischemic. Of course, since the vessel requires bypass in the first place there may have been little flow from it to the myocardium, thereby minimizing the effect of vessel occlusion. However, if that vessel provides sufficient flow to an area of viable heart muscle not supplied by collaterals, the heart may become rapidly ischemic during surgical repair. Systemic heparin (a dose of 100-300 units/kg but typically lower than the doses used for CPB, usually to a target activated clotting time of 250-300 s) is administered before vessel occlusion. Should efforts to support the circulation be inadequate during “off-pump” bypass the surgical team should be prepared for full heparinization and conversion to an on-pump approach. The CPB pump should be fully primed and on standby with the perfusionist in attendance for the case.
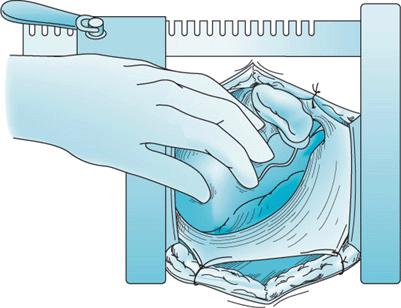
Figure 13–1A. During OPCAB surgery using a full sternotomy the heart is frequently lifted by the surgeon in the chest to gain exposure to the vessel to be bypassed.
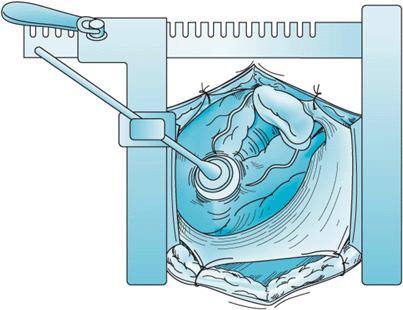
Figure 13–1B. Using stabilization devices, the heart is positioned to optimize surgical exposure and to provide a relatively still target for bypass graft placement.
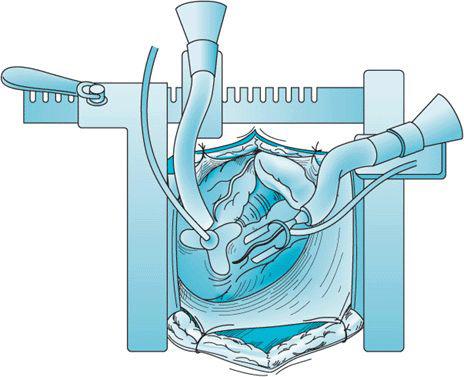
Figure 13–1C. With the heart positioned, the coronary artery to be bypassed is stabilized.
Surgeons have also attempted to use minimally invasive surgical techniques for valvular surgery. The femoral vessels are cannulated and using minimally invasive approaches the valves are repaired or replaced. Minimally invasive aortic valve surgery can be done through a ministernotomy. At times surgeons may request the anesthesiologist to aid with placement of a coronary sinus catheter from the internal jugular vein for the administration of retrograde cardioplegia. TEE is employed to position the catheter in the coronary sinus. The mitral valve can be approached through a minithoracotomy or a ministernotomy. Various thoracoscopic and robotic approaches have been tried to access the mitral valve using femoral bypass. Catheter based valve replacements have been previously discussed.
ANESTHETIC CHALLENGES FOR OFF-PUMP AND MINIMALLY INVASIVE SURGERY
Prior to establishing invasive arterial monitoring and central venous access, the anesthesiologist and the surgeon should discuss the surgical plan especially regarding which vessels will be cannulated for initiating CPB or whether the placement of a retrograde coronary sinus catheter through the internal jugular vein is necessary. If the case involves a ministernotomy with CPB cannulas placed in the chest, the procedure will unfold similarly to other procedures requiring a full sternotomy. Since a ministernotomy may not permit full access to the heart, external defibrillation/pacemaker pads must be placed if internal paddles are unable to properly make contact with the epicardium. External pacing may treat protracted severe bradycardia. Swan-Ganz catheters with pacing capabilities can be used to provide transvenous pacing if epicardial pacing is not considered feasible.
If the procedure is performed through a thoracotomy, the ability to provide one-lung ventilation is required. Double-lumen endotracheal tubes or bronchial blockers are used depending upon patient characteristics, anesthesiologist’s preference, and need for postoperative mechanical ventilation.
Choice of anesthetic agent for minimally invasive surgery parallels that of conventional cardiac surgery. Although high-dose narcotic-based anesthetics (eg, 50 μg/kg of fentanyl) can be used, anesthetics can be designed to provide fast track emergence and extubation in the operating room. Combinations of opioids (short-acting or carefully titrated longer-acting), inhalational agents, and propofol have all been used in these cases successfully. As with all cardiac anesthesia practice, careful management of the patient’s hemodynamics is far more important than the particular anesthetic method chosen. Some centers have even used regional anesthesia for off-pump bypass surgery (thoracic epidural anesthesia), although the authors do not advocate this approach.
Monitoring for minimally invasive procedures is similar to that employed in fully invasive cardiac surgery. In procedures performed through small incisions, the anesthesiologist often cannot see the beating heart, which can otherwise be a reasonable monitor of cardiac function. Therefore, TEE monitoring of heart function during minimally invasive procedures becomes even more important. However, when the heart is lifted from the chest to facilitate placement of a bypass grafts during off-pump surgery, TEE imaging becomes difficult and may not always be useful in detecting perioperative ischemia. When TEE images are available, the appearance of new wall motion abnormalities during coronary artery occlusion can signal the development of myocardial ischemia. Release of coronary arterial snares and the restoration of blood flow will usually resolve ischemia. Hypotension, increased pulmonary arterial pressures, new ST-segment changes, arrhythmias can all complicate off-pump surgical procedures. Surgical use of coronary shunts may at times relieve ischemia. Adequate volume loading, placement of the patient in Trendelenburg position may be helpful in increasing preload and may assist in cardiac displacement for access to the vessels to be grafted. Often vasopressors are given to support the blood pressure when the heart is lifted out of the chest or rendered ischemic by snare ligatures. Conversely, when the heart is returned to its normal position or ischemia relieved and cardiac output unimpeded, blood pressure can shoot up dramatically leading to unexpected hypertension.
As mentioned above, the surgical and anesthesia teams should be prepared at all times to convert the procedure from an off-pump minimally invasive procedure to a full sternotomy, on-pump procedure should hemodynamic instability ensue and should efforts to restore blood pressure and relieve surgically induced coronary ischemia falter.
Surgeons from time to time employ various transthoracic and intra-aortic cross clamps to isolate the heart from the systemic circulation when using “port-access” surgery in order to deliver cardioplegia. TEE is used in these situations to ensure that the intra-aortic balloon clamps do not become malpositioned in the aorta potentially occluding flow to the innominate artery. Aortic dissections can also be detected should they occur secondary to port access approach. Due to various surgical limitations, port-access surgery is rarely encountered today although was once hoped to become popular by reducing or eliminating fully invasive sternotomies.
Robotic approaches have been employed for coronary bypass and epicardial pacemaker lead placement. Although multivessel coronary artery bypass performed robotically was once thought likely, many operating room robots these days are used in urologic or gynecologic procedures rather than cardiac surgery. It is important that appropriate muscle paralysis is provided during robotic procedures, as the robotic arms are rather fixed and may cause trauma should the patient move or cough during surgery. Most robotic cases are done via a thoracotomy and will require lung isolation and one-lung ventilation.
Postoperatively, patients undergoing MIDCAB or OPCAB may be ideal candidates for early extubation in the operating room. Particular attention should be paid to adequate control of bleeding, correction of any existing coagulopathy, adequate control of pain, and maintenance of normothermia. The patient must be actively warmed throughout surgery and room temperature controlled. The usual blood gases and routine lab values should be monitored and corrected as with any cardiac surgery patient. Some centers, however, due to concern regarding the above mentioned factors (bleeding, pain, hemodynamic instability) might elect to keep the patient intubated and sedated for a short period of time prior to extubation in the ICU.
IS OFF-PUMP SURGERY BETTER THAN ON-PUMP SURGERY?
Considering the numerous inflammatory and coagulation derangements associated with cardiopulmonary bypass, it was hoped that off-pump techniques would reduce the complications associated with heart surgery—especially those related to neurologic injury. There have been a number of studies that have suggested or failed to suggest that off-pump techniques offer some advantages. Bucerius et al looking at a large database found a reduced incidence of postoperative stroke and delirium in patients who underwent beating heart surgery compared with those on CPB.3 On the other hand, Nahoe et al in a prospective trial of relatively healthy patients randomized to on- or off-pump surgery found no difference in cardiac surgery outcomes at 1 year including freedom from death, stroke, myocardial infarction, or additional coronary intervention.4 Khan et al randomized a small number of patients (roughly 50 in each group) to on- or off-pump surgery and assessed graft patency 3 months postoperatively.5 The investigators noted that although there was a lower degree of myocardial damage as measured by troponin T levels following off-pump surgery, graft patency was lower in off-pump patients compared to those operated using on-pump techniques. Since off-pump surgery is performed on the beating heart with the use of myocardial stabilization devices, it is possible that grafts performed under these conditions may be technically inferior, thus, have lower patency and longevity rates compared to those completed in the arrested heart following cardioplegia.
A very recent study in 2203 randomly assigned patients to undergo off-pump or on-pump revascularization, found that the off-pump group had worse outcomes (death or complications like reoperation, new mechanical support, cardiac arrest, coma, stroke, or renal failure before discharge or within 30 d from surgery) and poorer graft patency than did patients in the on-pump group. There were no significant differences between the techniques in neuropsychological outcomes or use of major resources.6
Cognitive dysfunction as measured using psychometric testing is present in up to 50% of patients following cardiac surgery. Interestingly, in the long term there appears to be little difference in the presence of cognitive dysfunction in on- versus off-pump cardiac patients.7 Of course, unlike stroke or delirium which are clinical diagnoses, cognitive dysfunction must be assessed before and after cardiac surgery by psychological testing. At times, these testing methods themselves have come into question, making assessments as to the benefit of off-pump surgery in this setting difficult.
At present the choice of surgical technique is in fact the choice of the surgeon. Different surgeons have varying experiences with off-pump procedures and that may determine the use of this approach in a given institution. Certainly, selective use of off-pump surgery using the internal mammary arteries without cross clamp of the aorta can be helpful when the aorta is highly calcified or the patient’s condition is especially susceptible to the deleterious effects from CPB. On the other hand, the patient with severe heart failure, cardiomegaly, and low ejection fraction may not permit manipulation of the heart or coronary artery occlusion by becoming too hemodynamically unstable to tolerate off-pump repairs.
Whenever off-pump techniques are to be employed communication between surgeon and anesthesiologist should be close. Lifting the heart to gain surgical exposure and the application of stabilization devices may affect hemodynamic performance. Snare ligature of coronary arteries can quickly result in myocardial ischemia and hemodynamic collapse. Likewise, the anesthesiologist should inform the surgeon if they must use heroic efforts to support the circulation in order for the patient to tolerate coronary occlusion or heart manipulation.
CASE SCENARIO
A 73-year-old man presents for coronary artery bypass grafting. He has a severely calcified aorta. What are his options?
Assuming that catheter-mediated PCI therapies have been ruled out, this patient is a candidate for off-pump surgery if he has no coexisting valvular disease in need of repair and can tolerate manipulations of the heart to facilitate completion of the graft anastomoses.
The surgeon lifts the heart to position it prior to completion of the first bypass graft. The blood pressure falls to 60 mm Hg systolic. How should the anesthesia team respond?
The anesthesiologist notes no new ST-T wave abnormalities and administers vasopressors and intravenous fluids and places the patient in slight Trendelenburg position to ensure adequate preload and offset the decrease in venous return. Blood pressure improves to 90 mm Hg systolic. Following heparinization and graft harvest, the surgeon places snares across the left circumflex artery. The patient remains hemodynamically stable. The anastomosis is completed uneventfully.
While completing the final bypass graft to the right coronary the patient becomes asystolic. What should be done now?
The surgeon places an epicardial pacemaker wire and temporary VVI pacing is begun. The bypass graft is completed and the rhythm restored. The patient recovers uneventfully. Had pacing not been possible using epicardial, transcutaneous, or transvenous techniques and the patient not responding to ACLS protocol for bradycardia, emergency institution of CPB would be required.
REFERENCES
1. Wasnick J, Acuff T. Anesthesia and minimally invasive thoracoscopically assisted coronary artery bypass: a brief clinical report. J Cardiothorac Vasc Anesth. 1997;11(5):552-555.
2. Wasnick J, Hoffman W, Acuff T, et al. Anesthetic management of coronary artery bypass via minithoracotomy with video assistance. J Cardiothorac Vasc Anesth. 1995;9:731-733.
3. Bucerius J, Gummert J, Borger M, et al. Stroke after cardiac surgery: a risk factor analysis of 16,184 consecutive adult patients. Ann Thorac Surg. 2003;75:472-478.
4. Nahoe H, van Dijk D, Jansen E, et al. A comparison of on-pump and off-pump coronary artery bypass surgery in low risk patients. NEJM. 2003;348(5):394-402.
5. Khan N, De Souza A, Mister R, et al. A randomized comparison of off-pump and on-pump multivessel coronary-artery bypass surgery. NEJM. 2004;350(1):21-28.
6. Shroyer AL, Grover FL, Hattler B, et al. On-pump versus off-pump coronary artery bypass surgery. NEJM. 2009;361(5):1827-1837.
7. van Dijk D, Jansen E, Hijman R, et al. Cognitive outcome after off-pump and on-pump coronary artery bypass graft surgery. JAMA. 2002;287(11):1405-1412.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


