34 Occipital Neuralgia∗
Anatomy
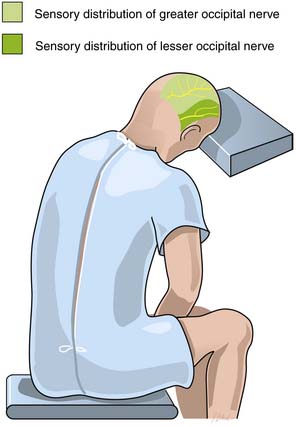
Occipital neuralgia is one type of cervicogenic headache described as pain in the distribution of the greater and/or lesser occipital nerve(s), associated with posterior scalp dysesthesia and/or hyperalgesia. The greater occipital nerve innervates the posterior skull from the suboccipital area to the vertex. It is formed from the medial (sensory) branch of the posterior division of the second cervical nerve.1 It emerges between the atlas and lamina of the axis below the oblique inferior muscle and then ascends obliquely on the latter muscle between it and the semispinalis muscle.1 The course of the greater occipital nerve does not appear to differ in males and females.2
The lesser occipital nerve forms from the medial (sensory) branch of the posterior division of the third cervical nerve, ascends similar to the greater occipital nerve, and pierces the splenius capitis and trapezius muscles just medial to the greater occipital nerve.1,2 It ascends along the scalp to reach the vertex, where it provides sensory fibers to the area of the scalp lateral to the greater occipital nerve. The Occipital neuralgia (for clarity) appears to be more common in females.3
Symptoms
Paroxysmal occipital neuralgia describes pain occurring only in the distribution of the greater occipital nerve. The attacks are unilateral, and the pain is sudden and severe. The pain is described as a lancinating, sharp, throbbing, electric shock-like pain.4–6 The pain may demonstrate a burning characteristic, but this is less common. Although single flashes of pain may occur, multiple attacks are more frequent. The attacks may occur spontaneously or be provoked by specific maneuvers applied to the back of the scalp or neck regions, such as brushing the hair or moving the neck.7
Two broad categories of patients with occipital neuralgia are those with structural pathology and those without apparent etiology.1 Proposed etiologies include myofascial tightening, trauma of C2 nerve root (whiplash injury), prior skull or suboccipital surgery, other type of nerve entrapment, idiopathic causes, hypertrophied atlantoepistrophic (C1-2) ligament, sustained neck muscle contractions, or spondylosis of the cervical facet joints (particularly C2-3 and C3-4).4,6,8–11 Most patients with occipital neuralgia do not have discernible lesions.1
Acute continuous occipital neuralgia often has an underlying etiology. The attacks last for many hours and are typically devoid of radiating symptoms (e.g., trigger zones to the face). The entire episode of neuralgia will continue up to 2 weeks before remission. Exposure to cold is a common trigger.7
In chronic continuous occipital neuralgia, the patient may experience painful attacks that last for days to weeks. These attacks are generally accompanied by localized spasm of the cervical or occipital muscles. The reported pain originates in the suboccipital region up to the vertex and radiates to the frontotemporal region. Radiation to the orbital region is also common. Sensory triggers to the face or skull can initiate a painful episode. Similarly, pain may increase with pressure of the head on a pillow. Prolonged abnormal fixed postures that occur in reading or sleeping positions and hyperextension or rotation of the head to the involved side may provoke the pain. The pain may be bilateral, although the unilateral pattern is more common. Often, a previous history of cervical or occipital trauma or arthritic disease of the cervical spine is obtained. Occasionally, patients may report other autonomic symptoms concurrently such as nausea, vomiting, photophobia, diplopia, ocular and nasal congestion, tinnitus, and vertigo.7 Severe ocular pain has also been described, as well as symptoms in other distributions of the trigeminal nerve.8,12–14 Convergence of sensory input from the upper cervical nerve roots into the trigeminal nucleus may explain this phenomenon.11
Entrapment of the nerve near the cervical spine may result in increased symptoms during flexion, extension, or rotation of the head and neck. Compression of the skull on the neck (Spurling’s maneuver), especially with extension and rotation of the neck to the affected side, may reproduce or increase the patient’s pain if cervical degenerative disease is the cause of the neuralgia.7 Pressure over both the occipital nerves along their course in the neck and occiput, or pressure on the C2-3 or C3-4 facet joints should cause an exacerbation of pain in such patients, at least when the headache is present. Even if the actual pathology is in the cervical spine, tenderness over the occipital nerve at the superior nuchal line is usually present.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


