CHAPTER 8 Obstetrics
Anaesthesia for non-obstetric surgery during pregnancy
In descending order of preference:
Regional anaesthesia
Epidurals give excellent/satisfactory analgesia in 91% of mothers. Increased use of regional techniques probably accounts for the continuing reduction in maternal mortality by avoiding risks of failed intubation and aspiration. Comparative Obstetric Mobile Epidural Trial (COMET) 2001 showed that women requesting analgesia for pain relief were more likely to require instrumental delivery if receiving 0.25% bupivacaine boluses rather than low dose bupivacaine infusion or combined spinal/epidural, but no significant difference in LSCS rates between groups (Table 8.1).
Table 8.1 Advantages and disadvantages of epidural anaesthesia
| Advantages | Disadvantages |
|---|---|
| Maternal participation at delivery | May take too long to perform if there is fetal distress |
| Avoids risk of failed intubation | Hypotension |
| Reduced risk of aspiration | Risk of patchy, incomplete block |
| Avoids morbidity from GA drugs | Backache |
| Avoids risk of awareness | Urinary retention |
| Earlier breast-feeding | |
| Good postoperative analgesia | |
| Less postnatal depression |
Pain pathways (Fig. 8.1)
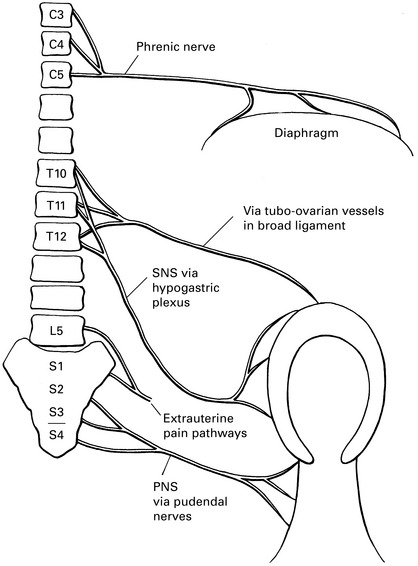
LSCS stimulates sensory nerves to T10 in addition to phrenic. Aim to block from T8 to S5.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


