Parameters of physical growth
Gross motor milestones
Fine motor milestones
Speech and language milestones
Cognitive and social-emotional milestones
2.0 cm/month during the first 3 months of life
1.0 cm/month during months 3 through 6 of life
0.5 cm/month from months 6 through 12
Large or small heads warrant close assessment to detect treatable problems (hydrocephalus, metabolic disturbances or syndromes, anatomic problems, congenital infections) and monitor development.
Large or small stature can be associated with a number of syndromes, including developmental delays (Soto syndrome and various chromosomal abnormalities).
Rolling before 3 months
Poor head control at 5 months
Lack of sitting by 9 months
Persistence of Moro reflex, asymmetric tonic neck reflex, and tonic labyrinthine reflex past 6 months
Lack of development of protective supportive reactions (e.g., lack of parachute response by 12 months)
Hand dominance before 18 months
Inability to walk independently by 18 months
TABLE 38.1 AVERAGE VALUES FOR PHYSICAL GROWTH PARAMETERS IN THE FIRST 2 YEARS OF LIFE | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
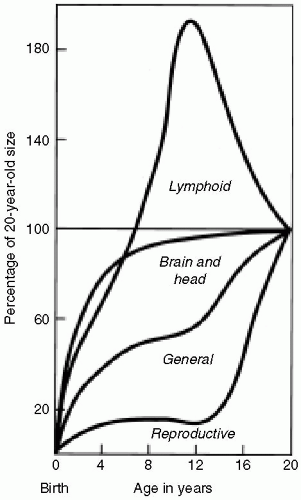 Figure 38.1 Growth patterns of various systems. (From Bickley LS, Hoekelman RA. Bates’s guide to physical examination and history taking, 7th ed. Philadelphia: Lippincott Williams & Wilkins, 1999:621, with permission.) |
3-year-old: circle
4-year-old: cross
4.5-year-old: square
5-year-old: triangle
language (receptive) are acquired by learning to localize sound. Expressive skills begin with cooing (vowel sounds) and differentiated crying when the baby is hungry, hurt, or in need of attention. At 3 months, babies begin vocalizing when they see an adult, and at 5 months, they take turns vocalizing with adults, quieting when the other speaks, and mimicking tone changes, although not actual words. At 6 months, babies add consonants (babbling), and when their parents respond to “mama” and “dada” with smiles and hugs, the baby eventually connects meaning to those sounds. When babies attach meaning to gestures or vocalizations, they have developed true words and initiated the naming period (10-18 months). Usually, “mama,” “dada,” the infant’s name, and “no” are the first recognized labels. Once begun, the growth of receptive language is rapid, and by 12 months, 100 words may be understood. One-step commands associated with a gesture can be understood by the child at 1 year of age, and the need for a gesture is lost in a few months. The development of expressive skills progresses more slowly, with most children having at least one true
word before their first birthday and most of their verbalization consisting of complicated multisyllabic consonant and vowel sounds with intonation changes, called jargon. By the end of the naming period, 18-month-old children use approximately 25 meaningful words spontaneously.
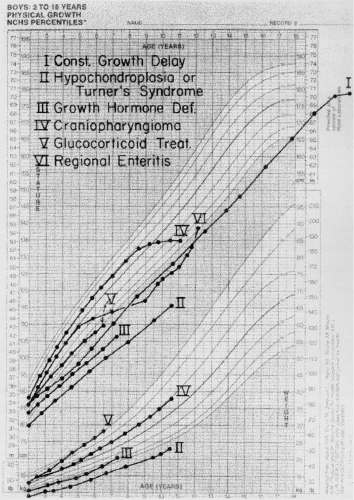 Figure 38.2 Growth patterns in children with short stature associated with six different causes. (From Kaplan SA. Clinical pediatric endocrinology, 2nd ed. Philadelphia: Saunders, 1990:51, with permission.) |
TABLE 38.2 GROSS MOTOR MILESTONES | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


