b. Reflexology involves the act of applying pressure to the “reflex” points on the feet and palms. Reflexology has not only been used for pain relief but also for treating nausea, vomiting, and fatigue in pregnancy. There has been relatively little research on the use of reflexology for labor pain. Dolatian et al.15 carried out a randomized controlled trial where parturients were randomly enrolled into three different groups. The first group received 40 minutes of reflexology at the beginning of the active phase. The second group received emotional support for the same duration at the same stage, and the third group received routine standard care. Pain intensity was found to be significantly lower in the reflexology group compared to the other two groups.15
CLINICAL PEARLCurrent evidence suggests that massage may be used as a pain relief measure in labor. More studies need to be done to evaluate the efficacy of reflexology in labor.
2. Hypnosis
a. Hypnosis is the induction of a deeply relaxed state in which a person loses the power of voluntary action and is highly responsive to suggestions. Once in this state, sometimes called a hypnotic trance, the patients are given therapeutic suggestions to encourage changes in behavior or relief of symptoms. “Hypnobirthing” has become a popular trend in recent years. Hypnobirthing programs teach women self-hypnosis, relaxation, and breathing techniques to help manage the stress and pain associated with labor. The anterior cingulate gyrus has been demonstrated on positron emission tomography to be one of the sites affected by the hypnotic modulation of pain.16
b. A Cochrane review of hypnosis included seven trials involving a total of 1,213 women. Six of the seven trials evaluated antenatal hypnotherapy. Only one trial provided hypnotherapy during labor. There were no significant differences between the hypnosis group and the control group for the primary outcomes: use of pharmacologic pain relief (average risk ratio [RR] 0.63; 95% CI, 0.39 to 1.01; six studies; 1,032 women), spontaneous vaginal birth (average RR 1.35; 95% CI, 0.93 to 1.96; four studies; 472 women), or satisfaction with pain relief (RR 1.06; 95% CI, 0.94 to 1.20; one study; 264 women).17 A large randomized controlled, single-blinded trial (1,222 healthy nulliparous women), carried out in Denmark, also did not find any differences in the use of epidural analgesia or pain experience across three study groups: a self-hypnosis group, a relaxation group, and a usual care group.18
CLINICAL PEARLBased on the current evidence, hypnosis cannot be recommended as an effective pain relief method in labor.
3. Aromatherapy
a. Aromatherapy is a complementary therapy using essential oils obtained from distillation of plant materials such as roots, leaves, bark, seeds, and flowers. Essential oils can be used through massage and aromatherapy diffusers or vaporizers. The two commonly used oils in labor are lavender and frankincense. Essential oils are thought to increase the body’s own sedative, stimulant, and relaxing substances.
b. A systematic review performed by Smith et al.19 included two trials (535 women) evaluating the use of aromatherapy in labor. The trials found no difference between the aromatherapy and control groups for the primary outcomes of pain intensity, assisted vaginal delivery, CD, and admission to neonatal intensive care unit.
CLINICAL PEARLThere is currently no strong evidence to support the effectiveness of aromatherapy in labor pain management.
4. Acupuncture and acupressure
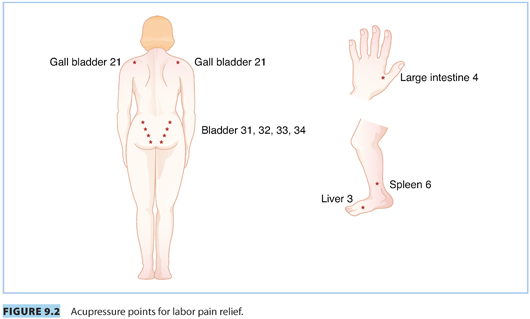
a. Acupuncture involves the insertion of various types of needles into the skin and subcutaneous tissues at specific points known as acupoints to correct the imbalance of energy in the body. It has been used for more than 2,000 years in China. For acupressure, the therapists use their hands and fingers to activate the same points as applied by acupuncture (see Fig. 9.2). Several theories have been presented to explain how acupuncture and acupressure may work. It has been proposed that acupuncture may modify the perception of pain.20 Other theories suggest that acupuncture stimulates the release of endorphins and opioids.21,22 Intrapartum acupuncture is usually provided by professional acupuncturists. In countries such as Germany and Denmark, it is widely performed by midwives.23
b. Chen et al.24 reviewed the studies on the use of acupuncture in labor over a 10-year period (2002 to 2012) in mainland China. There were 20 randomized controlled trials and 2 nonrandomized controlled trials. All studies found that acupuncture significantly relieved the pain during delivery.24 A Cochrane review by Smith et al.25 included 13 trials involving 1,986 women for their meta-analysis evaluating acupuncture or acupressure for the labor pain management. Nine trials reported on acupuncture and four trials studied acupressure. Reduced pain intensity was found in the acupuncture group when compared with the group which received no intervention (SMD −1.00; 95% CI, −1.33 to −0.67; one trial; 163 women). Another trial reported greater satisfaction with pain relief compared to the placebo control group (RR 2.38; 95% CI, 1.78 to 3.19; 150 women). A reduction in the use of pharmacologic analgesia was found in one trial, which compared acupuncture with placebo (RR 0.72; 95% CI, 0.58 to 0.88; 136 women). Pain intensity was reduced in the acupressure group when compared with the placebo control group (SMD −0.55; 95% CI, −0.92 to −0.19; one trial; 120 women) and the combined control group (placebo and no treatment) (SMD −0.42; 95% CI, −0.65 to −0.18; two trials; 322 women).25
CLINICAL PEARLCurrent evidence suggests that acupuncture and acupressure may be useful for the management of labor pain.
E. Hydrotherapy
1. Hydrotherapy, in the form of immersion in the birthing pool or bath, is used worldwide to promote relaxation and to reduce pain and anxiety in laboring women. For women without any antenatal or intrapartum complications, hydrotherapy is deemed to be safe.26 Immersion is associated with decreases in neuroendocrine responses in healthy adults. At a thermoneutral temperature of 34.5°C, during rest and exercise, immersion has been associated with decreases in levels of plasma norepinephrine27 and epinephrine.28 The National Institute for Health and Care Excellence29 guideline, published in 2007, recommended that the temperature of the woman and the water should be monitored every hour to ensure that the woman is comfortable and not febrile. The temperature of the water should not be above 37.5°C.
2. Nutter et al.30 published an integrated analysis of peer-reviewed literature on water birth in 2014. Thirty-eight studies, including 2 randomized controlled trials and 36 observational studies, were reviewed. Their aggregate results found that water birth was associated with high levels of maternal satisfaction with pain relief. It was also linked to decreased incidence of episiotomy and severe perineal tears. Neonatal mortality rates were found to be low and similar in women who used water immersion during labor and those who did not use water immersion. Another review included 12 trials (3,243 women).31 Results for the first stage of labor showed that there was a significant reduction in the epidural, spinal, and paracervical analgesia use among the women allocated to water immersion compared to the controls (478 of 1,254 vs. 529 of 1,245; RR 0.90; 95% CI, 0.82 to 0.99; six trials). There were no differences in the rates of assisted vaginal deliveries (RR 0.86; 95% CI, 0.71 to 1.05; seven trials), cesarean deliveries (RR 1.21; 95% CI, 0.87 to 1.68; eight trials), perineal trauma, or maternal infection. There were also no differences for Apgar scores less than seven at 5 minutes (RR 1.58; 95% CI, 0.63 to 3.93; five trials), neonatal unit admissions (RR 1.06; 95% CI, 0.71 to 1.57; three trials), or neonatal infection rates (RR 2.00; 95% CI, 0.50 to 7.94; five trials). However, there is considerable heterogeneity for some outcomes in this review. Authors recommended further research to be done.
F. Transcutaneous electrical nerve stimulation
1. Transcutaneous electrical nerve stimulation (TENS) is a technique whereby low-voltage pulsatile electrical impulses, varying in frequency and intensity, are administered through electrodes. For pain in the first stage of labor, electrodes are usually placed 2 cm over the T10–L1 dermatomes on either side of the spinous processes. A second set of electrodes is placed over the S2–S4 dermatomal areas for the pain relief in the second stage. The mechanism of action of TENS is based on the gate control theory of pain (see Fig. 9.1).11 It has also been reported that there are marked increases in β-endorphin and met-enkephalin with low-frequency TENS.32
2. A review of 14 studies involving 1,256 women found that there was little difference in satisfaction with pain relief or in pain ratings between TENS and control groups. On the other hand, women receiving TENS to acupuncture points were less likely to report severe pain (RR 0.41; 95% CI, 0.32 to 0.55).33 In a Cochrane review involving 25 studies, Dowswell et al.34 reported that there was little difference in pain ratings between the TENS and control groups. The majority of women, who used TENS, reported that they would use it again in a future labor.33
CLINICAL PEARLThere is no current evidence that TENS has any beneficial effect in treating labor pain.
G. Sterile water injection
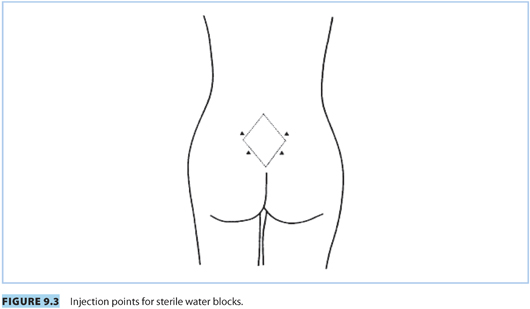
1. A sterile water injection is a simple technique to treat back pain in labor. It involves an intradermal injection of sterile water in the lumbosacral area (see Fig. 9.3). A small bleb is formed by injecting approximately 0.1 mL of sterile water. The optimal number of injection(s) is unknown. The mode of action is unclear. It is probably a form of counterirritation, invoking the gate control theory of pain.11 It has also been proposed that it may exert its effect through “physiologic distraction.”35
2. Derry et al.35 performed a systematic review evaluating seven randomized, double-blind, controlled studies on the use of intracutaneous or subcutaneous injection of sterile water for labor pain. All studies reported a greater reduction in pain in the sterile water injection group. However, due to the failure to demonstrate a normal distribution for pain intensity or relief and the use of different pain measurement scales, a meta-analysis of available studies was deemed inappropriate. One study found that significantly more women had “4/10 cm or more reduction” in pain with sterile water (50% to 60%) than with the placebo (20% to 25%). There was no significant difference between sterile water and saline for rates of CD (RR 0.58; 95% CI, 0.33 to 1.02), instrumental delivery (RR 1.31; 95% CI, 0.79 to 2.18), rescue analgesia (RR 0.86; 95% CI, 0.44 to 1.69), timing of delivery, or Apgar scores.35
CLINICAL PEARLSterile water injection should not be recommended to women in active labor.
II.Non-neuraxial pharmacologic methods of pain relief
A. Inhalation techniques
Inhalational analgesia is provided by intermittent inhalation of subanesthetic concentrations of volatile agents. The mother should remain conscious with preservation of her laryngeal reflexes, thereby avoiding regurgitation and aspiration of stomach contents. The technique first achieved fame and later gained widespread acceptance when John Snow administered chloroform to Queen Victoria for the birth of her eighth and ninth children in 1853 and 1857. A variety of anesthetic agents have been used over the years. Nitrous oxide has remained the most popular inhalation agent for labor pain relief. Other volatile agents, such as sevoflurane, have also been evaluated for the use in labor.
Inhalational agents can readily cross the placenta and the concentration in fetal blood soon approaches that of the mother. However, these agents are eliminated almost entirely through the mother’s lungs. Environmental pollution from unscavenged gases may be significant. The occupational risk of health care staff, who have regular exposure to subanesthetic concentration of volatile gases, is unknown.
1. Nitrous oxide
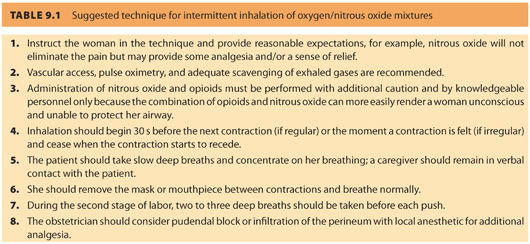
a. Nitrous oxide analgesia is administered as 50% nitrous oxide in oxygen using a blender device or via a premixed single cylinder. The blender device or cylinder is usually attached to a demand valve, which in turn, is connected to a face mask or mouthpiece. The demand valve only opens when the user applies negative pressure by inhaling through a mouthpiece or face mask (see Table 9.1). There is no flow from the system when the device is not in use. The incidence of its use for labor pain relief is 1% (or less) in the United States, 43% in Canada, and 62% in the United Kingdom.36 Obstetric anesthesiologists in the USA have expressed concerns about the effect of nitrous oxide on fetal neurodevelopment and its effects on the environment.36 Nitrous oxide acts on several types of receptors.37 It has an inhibitory action at N-methyl-D-aspartate (NMDA) glutamate receptors and has stimulatory activity at dopaminergic, α1-and α2-adrenergic, and opioid receptors. Common maternal side effects include nausea, dizziness, paresthesias, and dry mouth. It appears to be safe for the fetus.
b. Likis et al.38 published a systematic review evaluating the use of nitrous oxide for the management of labor pain. Although the authors identified 58 publications, only 2 of them were of good quality. Nitrous oxide was found to be less effective at relieving labor pain than epidural analgesia. Many mothers reported unpleasant side effects such as nausea, vomiting, dizziness, and drowsiness. Apgar scores of the babies, who were born to the mothers who used nitrous oxide, were not significantly different from those whose mothers used other forms of labor analgesia or no analgesia. Another review looked into the use of inhaled analgesia for pain management in labor and included 26 studies randomizing 2,959 women.39 Flurane derivatives were found to offer superior pain relief when compared to nitrous oxide in the first stage of labor as measured by a lower pain intensity score. The incidence of nausea was found to be higher in the nitrous oxide group when compared with the flurane derivatives group (RR 6.60; 95% CI, 1.85 to 23.52; two studies; 98 women). Placebo or no treatment was found to offer less pain relief compared to nitrous oxide (average RR 0.06; 95% CI, 0.01 to 0.34; two studies; 310 women). However, the nitrous oxide group had more side effects such as nausea (RR 43.10; 95% CI, 2.63 to 706.74; one study; 509 women), vomiting (RR 9.05; 95% CI, 1.18 to 69.32; two studies; 619 women), dizziness (RR 113.98; 95% CI, 7.09 to 1833.69; one study; 509 women), and drowsiness (RR 77.59; 95% CI, 4.80 to 1254.96; one study; 509 women) when compared with placebo or no treatment.
CLINICAL PEARLCurrent evidence suggests that nitrous oxide is an effective form of pain relief when compared to placebo, although many women will suffer unpleasant side effects. The potential for an adverse impact of nitrous oxide on fetal neurodevelopment, and on the environment, requires further research.
2. Volatile anesthetic agents
Volatile anesthetic agents have been studied for labor analgesia. They are more effective in reducing pain intensity in labor when compared to nitrous oxide.39 However, there has not been widespread use of these agents. Their routine use is limited by the need for the anesthesiologist’s presence, concerns for environmental pollution, potential for maternal amnesia, and the loss of protective airway reflexes. All volatile agents also cause dose-dependent uterine smooth muscle relaxation.
a. Sevoflurane has a low blood gas partition coefficient (0.65), allowing rapid onset and offset of action. It also has a less unpleasant odor when compared with other volatile anesthetic agents. Yeo et al.40 carried out an open-labeled escalating-dose study involving 22 laboring women. Sevoflurane was self-administered using an Oxford Miniature Vaporizer (OMV). The inspired concentration was increased by 0.2% after each contraction and decreased when sedation occurred. Pain relief scores did not increase significantly above inspired concentrations of 0.8% while sedation continued to increase, with excessive sedation occurring at 1.2% sevoflurane. The authors concluded that the optimal inspired sevoflurane concentration for labor was 0.8%. The same research group published a second study in which they compared self-administered sevoflurane 0.8% with nitrous oxide in 32 laboring women.41 Each parturient underwent two open-label, three-part sequences in oxygen (50:50 mix) in random order (nitrous oxide/oxygen-sevoflurane-nitrous oxide/oxygen or sevoflurane-nitrous oxide/oxygen-sevoflurane). Pain relief scores were significantly higher for sevoflurane (median 67, interquartile range [IQR] 55 to 74, total range [TR] 33 to 100 mm) than for nitrous oxide/oxygen (median 51, IQR 40 to 69.5, TR 13 to 100 mm, P < .037). Nausea and vomiting were more common in the nitrous oxide/oxygen group (relative risk 2.7; 95% CI, 1.3 to 5.7; P = .004). No other adverse effects were observed in the mothers or babies.
b. Enflurane. McGuinness and Rosen42 compared the administration of 1% enflurane in air to nitrous oxide during the first stage of labor. Lower pain scores and a higher level of drowsiness were observed in the enflurane group. There has not been any recent study evaluating the effect of enflurane for labor analgesia.
c. Isoflurane. The use of 0.25% isoflurane and 50% nitrous oxide mixture was studied in 221 laboring women. It was found that nitrous oxide alone did not provide adequate analgesia. Although none of the mothers became sedated, the requirement for neonatal resuscitation was higher in mothers who had received systemic analgesia within 5 hours of birth in addition to the inhaled mixture.43
d. Desflurane. When the inhalation of 1% to 4.5% of desflurane was compared with 30% to 60% of nitrous oxide in oxygen in 80 healthy parturients, analgesia scores were similar in both groups. However, the incidence of amnesia was greater in the desflurane group (23% vs. 0%; P < .05).44
CLINICAL PEARLSevoflurane may be the best volatile agent for inhalation analgesia because it has fast onset and offset times and is also less irritating to the airway. However, like other volatile agents, its use is limited by the requirement for specialized equipment and trained personnel as well as its potential for causing uterine smooth muscle relaxation.
B. Non-opioid analgesia and sedatives
Non-opioid analgesia and sedatives have been used in early labor for mild to moderate pain. Due to maternal sedation and neonatal depression, sedatives are used very infrequently.
1. Acetaminophen
a. Acetaminophen is a first-line treatment for mild pain and pyrexia. It also plays an important role in multimodal analgesia. Acetaminophen is a weak inhibitor of both cyclooxygenase (COX)-1 and COX-2 receptors. Oral and rectal administration can produce analgesic effects within 40 minutes, with a maximal effect at 1 hour. However, bioavailability ranges from 63% to 89% for the oral form and 24% to 98% for rectal administration. The intravenous acetaminophen administration improves the bioavailability and speed of onset.
b. A triple-blind, randomized, placebo-controlled trial, involving 120 low-risk laboring women, compared the effect of 1,000 mg intravenous acetaminophen with intravenous sterile water.45 When compared to the control group, the acetaminophen group was associated with lower visual analogue scale (VAS) score at 15 and 30 minutes after the start of medication. There was also a lower need for rescue medication (8 of 57 [14%] vs. 49 of 59 [83.1%], P < .001) at 60 minutes. There were no differences in the incidence of intrapartum fetal distress or neonatal Apgar scores between two groups. Another study involving 102 women compared the efficacy of acetaminophen to that of meperidine and reported that the reduction in pain was significantly greater in the meperidine group only at 15 minutes. However, none of the women in the acetaminophen group had adverse effects, as compared with 64% of the meperidine group.46 In summary, acetaminophen is a safe analgesic drug to be used for labor pain. However, more studies need to be done to compare it with other forms of labor analgesia.
2. Ketamine
a. Ketamine is a phencyclidine derivative and acts primarily by noncompetitive antagonism at the NMDA receptors. It can be given either intravenously or intramuscularly. When given intravenously, it has an onset of action within 30 seconds and duration of action between 5 and 10 minutes. If an intramuscular route is used, it has an onset within 2 to 8 minutes with duration of action of 10 to 20 minutes. It is metabolized in the liver, and active metabolites are excreted in the urine. Its use is limited by its adverse psychological effects. It can also cause an increase in heart rate and blood pressure. Therefore, it should be avoided in parturients with preeclampsia or hypertension.
b. There have not been many studies of ketamine for labor analgesia. Joel et al.47 performed a double-blind, randomized, placebo-controlled trial, which compared low-dose intravenous ketamine infusion with a normal saline control infusion for labor pain. The study showed that a low-dose ketamine infusion (loading dose of 0.2 mg per kg delivered over 30 minutes, followed by an infusion at 0.2 mg/kg/h) provided acceptable analgesia during labor. Although there was no significant clinical change in the maternal hemodynamics and fetal heart rate, 48.5% of women had transient light-headedness in the ketamine group. All the neonates in both groups were successfully breastfed. The umbilical cord blood pH was between 7.1 and 7.2. Overall maternal satisfaction was found to be significantly higher in the intervention group.47 There is a need for more studies to be done to compare the efficacy of ketamine with other conventional methods of pain relief.
3. Sedatives
Sedative agents, such as benzodiazepines, phenothiazines, and barbiturates, have been used in labor as adjuncts for pain relief and as anxiolytics. Most of these agents can readily cross the placenta and cause significant side effects for both the mother and the neonate. Their use is generally not recommended.
a. Benzodiazepines, such as diazepam, lorazepam, and midazolam, have been used in labor as adjuncts for analgesia.
(1) Benzodiazepines act by binding to a specific receptor site on γ-aminobutyric acid (GABA) receptors, facilitating their transmission. Midazolam has the fastest elimination half-life, followed by lorazepam and then diazepam (1 to 4 hours, 10 to 20 hours, and 20 to 45 hours, respectively). They cross the placenta easily. They are associated with significant side effects for both the mother and the baby, such as maternal and neonatal respiratory depression and neonatal hypotonicity and impaired thermoregulation.
(2) McAuley et al.48 randomized 50 primigravid mothers into a lorazepam (2 mg) group or placebo group. Meperidine 100 mg was given as required. Analgesia was significantly better in the lorazepam group. However, there was a higher incidence of respiratory depression in the neonates born to the mothers who received lorazepam. A higher incidence of amnesia was also observed in the mothers in the lorazepam group. Evidence for the use of benzodiazepines is limited. It is generally not advisable to use them as adjuncts for pain relief in labor, but they can be useful for women who have a severe panic attack during labor.
b. Phenothiazines (e.g., promethazine and chlorpromazine) have been used in the past for labor pain. They are dopamine antagonists with sedative, antiemetic, and antipsychotic properties. They can readily cross the placenta. They have many unwanted side effects, such as mild respiratory depression, hypotension, and extrapyramidal movements in the mother and decreased heart rate variability in the fetus.
c. Barbiturates are anesthetic agents that act mainly on GABA receptors to cause sedation. They have been used in early labor to reduce anxiety. They can readily cross the placenta and cause neonatal depression.
CLINICAL PEARLAcetaminophen and ketamine have not been adequately evaluated for labor analgesia. Sedatives are to be avoided unless specifically indicated.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


