II. Peripheral nervous system. The peripheral nervous system (PNS) encompasses all nerves outside of the brain and spinal cord. The locations of these nerves, as well as their extensive number, make them particularly prone to injury by surgery, trauma, or entrapment. Peripheral nerves have the benefit of regeneration and regrowth, but this is not always perfect and may result in neuropathic pain. Surgical treatment ranges from decompression to excision [1].
A. Peripheral nerve decompression
1
1. Indications. Surgical decompressions are used to treat peripheral nerve entrapments. Where nerves are usually compressed in areas where they rest in superficial locations or are confined in small anatomic spaces. The pressure from the compression results in axonal degeneration and ischemic changes that may result in pain and motor weakness. The goal of surgery is to relieve the compression [2].
2. Common nerve entrapments
a. Carpal tunnel syndrome. Carpal tunnel syndrome is the most common nerve entrapment and results from compression of the median nerves between the bones of the wrist and the flexor retinaculum that make up the carpal tunnel. Symptoms include pain in the first three fingers of the hand that is often worse at night, with weakness in the thumb [3].
b. Cubital tunnel syndrome. Cubital tunnel syndrome is the second most common nerve entrapment and results from entrapment of the ulnar nerve at the elbow. Patients may have symptoms of pain in the last two digits of their hand and weakness in their intrinsic hand muscles [4].
c. Suprascapular nerve entrapment. The suprascapular nerve travels through the suprascapular notch beneath the suprascapular ligament. Compression of this nerve by the ligament can result in shoulder pain with radiation to the shoulder blades as well as weakness in abduction and external rotation of the shoulder [5].
d. Piriformis syndrome. The sciatic nerve travels anterior to the piriformis muscle but can travel posterior, or even through this muscle, that can result in entrapment of the sciatic nerve. Entrapment can also be caused by muscular hypertrophy or repeated trauma [6]. Symptoms include buttock pain that radiates down the back of their leg [7]. Patients may also have knee weakness. Piriformis syndrome can be hard to differentiate from a lumbar radiculopathy.
e. Thoracic outlet syndrome. Thoracic outlet syndrome can also be difficult to diagnose. This syndrome involves compression at the thoracic inlet of the neurovascular bundle that consists of the brachial plexus, subclavian vein, and artery [8]. Compression may be of any of these structures with the most common compression being of the brachial plexus. This compression can occur in multiple areas including the interscalene triangle, between the clavicle and first rib, or at the attachment of the pectoralis minor [9]. Some patients also have a cervical first rib which may also cause compression of the neurovascular bundle.
(1) Surgical approach toward thoracic outlet syndrome depends on the structures involved in the entrapment. These may include resection of the first rib or cervical rib, anterior scalene muscle, or resection of the costoclavicular ligament [10]. This procedure can be done by either a transaxillary or supraclavicular approach.
3. Anesthetic considerations. Nerve entrapments are associated with a higher incidence of endocrine diseases. Approximately 15% of these patients may have diabetes [1]. Acromegaly is associated with nerve entrapment as well as obesity and pregnancy [11,12]. Other comorbid conditions associated with nerve entrapments include rheumatoid arthritis, gout, amyloidosis, and carcinomatosis.
CLINICAL PEARL
Neuropathies are associated with a higher incidence of endocrine diseases including diabetes, in addition to other comorbid conditions like acromegaly, obesity, rheumatoid arthritis, gout, amyloidosis, and carcinomatosis.
a. Many different anesthetic techniques have been used successfully. It is presently controversial to perform a regional or neuraxial technique in patients who may have pre-existing nerve injury. A thorough physical examination and documentation of pre-existing nerve injury should be done prior to any anesthetic and the risks and benefits of each technique should be weighed.
b. With any pain in patients, postoperative pain management can be a challenge. This is particularly so in patients receiving rib resections for their thoracic outlet syndrome since this can be a painful procedure. Paravertebral blocks for postoperative pain control in first rib resections have been successful and may be considered [13]. Other anesthetic concerns include the potential for rapid blood loss as well as the inability to trust or use the affected limb for blood pressure or IV access.
B. Neurectomy. A neurectomy may be performed to treat a number of conditions. One intention is to denervate a painful area, providing symptomatic relief to the patient. Another may be to remove an aberrantly firing nerve that is thought to be the pain generator. This may be a previously injured nerve that has formed a painful neuroma and excision allows the nerve to heal, forming a new neuroma that may not be as painful [14].
1. Patient characteristics. Patients presenting for a neurectomy may have a prior history of nerve injury, surgery, or trauma that resulted in nerve injury. They may present with symptoms of burning, shooting pain in the distribution of a peripheral nerve or in the area of a neuroma with signs of allodynia, dysesthesia, or hypoesthesia. These patients may have undergone conservative treatment with neuropathic pain medications or diagnostic procedures including nerve blocks to help identify the abnormal nerve [1].
a. Another type of patient undergoing a neurectomy is one with localized disease, either joint disease from osteoarthritis or visceral disease from a malignancy that results in severe pain. The goal of the neurectomy is to denervate the sensory input from the painful areas.
2. Common indications
a. Intercostal neuralgia. This may be caused by chest trauma or a prior thoracotomy. A neurectomy can be performed through a video-assisted thorascopic (VATS) procedure or through an open procedure [15].
b. Meralgia paresthetica. This is the result of either entrapment or injury to the lateral femoral cutaneous nerve, and the nerve can be transected surgically if decompression is not helpful [16].
c. Morton’s neuroma. This is compression of a digital nerve in the foot causing swelling of the digital nerve resulting in pain with walking and wearing shoes. Though not a true neuroma, surgical excision may provide pain relief [17].
d. Cancer pain. Neurolysis of the celiac plexus is commonly performed for treatment of painful upper abdominal malignancies. The superior hypogastric plexus can also be neurolysed for pelvic malignancies, either percutaneously or through an open procedure with direct visualization of the nerves.
e. Neuroma excision. Painful neuromas can be excised and while they may grow back, relocation may provide pain relief. One of the most common areas for this is in amputation stumps which may contain multiple neuromas causing stump pain.
C. Dorsal rhizotomy. This procedure involves surgical resection of the dorsal root and the dorsal root ganglion to denervate a painful sensory dermatome [18].
1. Indications. This procedure is no longer commonly performed, but has been used to treat intercostal neuralgia, angina, and visceral pain. It is generally reserved for individuals with pain in an area corresponding to one dermatome. There may be a high recurrence rate for pain which may not have been seen in the studies that examined cancer pain treatment [19].
2. Technique. This procedure is performed either through a laminectomy, intradurally, or by resecting a facet and approaching the nerve through an extradural approach. Multiple levels may need resecting due to the dermatome overlap since multiple nerve roots provide small contributions to each dermatome [20].
D. Sympathectomy. The sympathetic nervous system has multiple connections with sensory afferents and in some pain disorders it may contribute to the maintenance of the painful sensory input. In this sympathetically maintained pain, a sympathectomy may help provide pain relief [21].
2
1. Indications. A surgical sympathectomy for pain is reserved for sympathetically maintained pain syndromes that are refractory to nonsurgical treatments. Patients may show signs of sympathetic nervous system involvement including vasomotor and pseudomotor changes in the affected area. They are usually diagnosed with a sympathetic blockade which provides significant pain relief.
2. Surgical approach. The surgical approach is highly dependent on the area of the sympathetically maintained pain. For treatment of the upper extremity, the upper thoracic sympathetic ganglia need to be removed. This is most commonly done thorascopically, but can also be done through a superclavicular transaxillary or posterior costotransversectomy approach. The lumbar sympathetic chain can be accessed with an anterolateral retroperitoneal approach [22].
3. Anesthetic considerations. The surgical approach should be discussed with the surgeon given the possible need for one-lung ventilation to gain access to the thoracic sympathetic chain. Patients may develop hypotension that is generally transient. They may also have transiently increased gastrointestinal motility and may develop postsympathectomy pain characterized by burning or deep aching pain with hyperalgesia, though the onset does not usually occur for a few weeks postoperatively [23].
CLINICAL PEARL
After sympathectomy, patients may develop transient hypotension, increased gastrointestinal motility, and postsympathectomy pain.
3
E. Trigeminal neuralgia. This is a disorder of the trigeminal nerve that results in paroxysmal lancinating pain in the trigeminal nerve distribution that lasts a few seconds to minutes and is precipitated usually by a tactile stimulus. It is associated with compression of the trigeminal nerve by another nerve or an artery, and is commonly treated with microvascular decompression surgery.
1. Surgical technique. This procedure is done as a craniotomy with the incision located retroauricular at the mastoid process. Patients are generally positioned in a lateral park bench position. The goal of surgery is to dissect the compressing vessel off the trigeminal nerve [24].
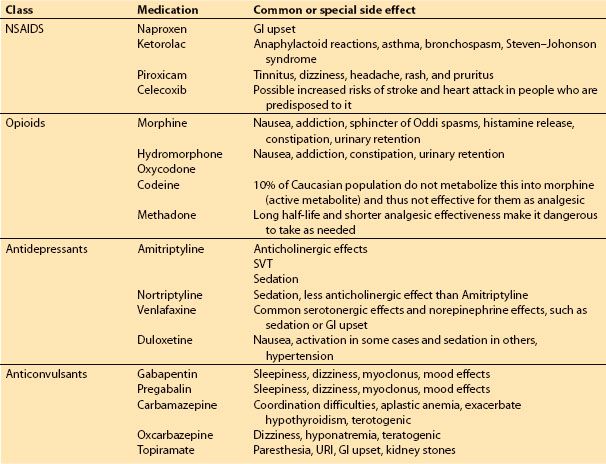
2. Anesthetic considerations. Patients may be on multiple antiepileptic or neuropathic medications that may have significant side effects and drug interactions (see Table 11.2). Operative location is in close proximity to a transverse sinus putting these patients at higher risk for massive blood loss or an air embolus.
Table 11.2 Commonly used neuropathic pain medications and their side effects
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


