The principal pharmacologic effect of neuromuscular-blocking drugs (NMBDs) is to interrupt transmission of synaptic signaling at the neuromuscular junction (NMJ) by interacting with the nicotinic acetylcholine receptor (AChR).
I. NEUROMUSCULAR JUNCTION
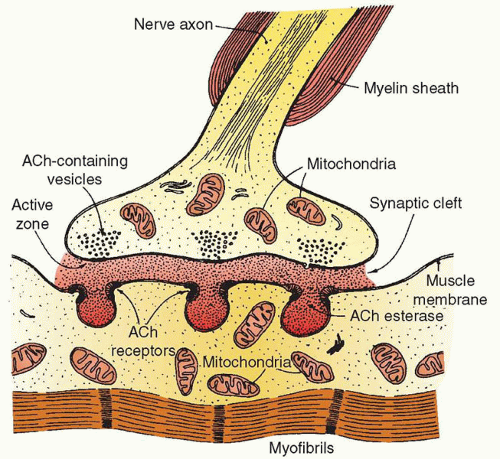
A. The NMJ (Fig. 13.1) is a chemical synapse located in the peripheral nervous system. The NMJ is composed of the neuronal presynaptic terminal, where acetylcholine (ACh) is stored in specialized organelles known as synaptic vesicles, and the postsynaptic muscle cell (motor endplate), where high densities (up to 10,000/µm2 at the synapse) of the nicotinic AChRs are found.
B. In response to an action potential in the nerve, voltage-dependent calcium channels, which are highly concentrated in close proximity to synaptic vesicles, open and cause a rapid influx of calcium into the nerve terminal increasing its intracellular concentrations to approximately 100 µM. This influx of calcium lasts only about 0.5 milliseconds but is sufficient enough to induce fusion of synaptic vesicles with the plasma membrane to release stored ACh. ACh then diffuses across the synaptic cleft where two molecules of ACh bind to a single nicotinic AChR.
C. Postjunctional nicotinic AChRs are glycoproteins composed of five subunits (two α and one each of β, δ, and ε) with the two α-subunits constituting the binding sites for ACh and NMBDs. When two molecules of ACh are bound, the AChR undergoes a conformational change (activation) that allows influx of sodium and calcium into the muscle cell to depolarize the membrane and causes contraction. Once depolarization occurs, repolarization begins with the efflux of potassium and the cessation of sodium and calcium entry. At this point, the AChR becomes inactivated. The amount of ACh released and the number of postsynaptic AChRs is much greater than that actually needed to induce contraction. This is termed the “safety factor” for neuromuscular transmission and plays a crucial role in certain pathologic conditions. After triggering depolarization, ACh diffuses into the synaptic cleft where it is rapidly hydrolyzed (within 15 milliseconds) by acetylcholinesterase (AChE) into choline and acetate. Choline is subsequently recycled to synthesize new ACh in the motor nerve terminal.
D. Prejunctional nicotinic AChRs are located on the presynaptic nerve terminal and are responsible for augmenting depolarization of the nerve terminal during high frequency stimulation, thereby enhancing ACh release. Antagonism of these receptors by nondepolarizing NMBDs is the mechanism by which these agents produce fade on the train of four (TOF).
II. GENERAL PHARMACOLOGY
A. Cholinergic receptors are categorized as nicotinic and muscarinic by their responses to the alkaloids nicotine and muscarine, respectively. There are two main classes of nicotinic cholinergic receptors, muscular ( found at the NMJ) and neuronal ( found in autonomic ganglia, at end-organ sites of parasympathetic nerves, and in the central nervous system). Since the cholinergic receptors have different subunit composition, most drugs bind to them with different affinity and have different effects. Only ACh and drugs working by producing ACh (AChE inhibitors) are agonists at all of them.
FIGURE 13.1 The neuromuscular junction.
B. There are well-described signaling systems that regulate the distribution and density of AChRs at the NMJ. Pathologic conditions that affect AChR distribution are quite common. For example, denervation, prolonged inactivity, or prolonged mechanical ventilation decreases the density of AChRs at the NMJ, whereas extrajunctional AChRs (often referred to as immature or fetal postjunctional nicotinic AChRs) proliferate over the surface of the muscle membrane. This “up-regulation” of AChRs increases sensitivity to agonists such as ACh and succinylcholine, but it decreases the sensitivity to competitive antagonists such as nondepolarizing NMBDs. In contrast, increased sensitivity to antagonists and decreased sensitivity to agonists develop under conditions associated with down-regulation of AChRs. This can occur when the NMJ is exposed to excess ACh (e.g., following chronic use of AChE inhibitors).
C. NMBDs can be classified by the duration of effect: ultrashort-acting (<10 minutes; succinylcholine), short-acting (<20 minutes; mivacurium [not available in the United States]), intermediate-acting (45 to 60 minutes; atracurium, cisatracurium, rocuronium, and vecuronium), and longacting (>1 hour; pancuronium). Nondepolarizing NMBDs can be further classified by chemical class: aminosteroid derivatives (e.g., pancuronium, rocuronium, and vecuronium) and benzylisoquinolines (e.g., atracurium, cisatracurium, and mivacurium). NMBDs differ substantially in their onset, duration of blockade, metabolism, side effects, and interactions with other drugs (Tables 13.1 and 13.2).
TABLE 13.1 Comparative Clinical Pharmacology of NMBDsa
aThere is a large variability in the response to all relaxants, especially at the extremes of age and with profound illness. Therefore, all patients should be carefully monitored as described in the text. Doses shown here are intended for intravenous administration in adult patients.
b An ED95 dose of a relaxant provides adequate surgical relaxation with nitrous oxide-opioid anesthesia.
c These are customary intubating doses and not all equipotent. Neuromuscular blockade is potentiated by volatile anesthetics. For nondepolarizing agents, the intubating dose can be approximately double of the ED95.
d These times reflect the use of customary intubating doses and may be substantially altered by the depth of anesthesia. For a rapid sequence induction with nondepolarizing agents, onset time can be shortened by administering a priming dose 3-5 minutes before the full dose. Alternatively, a dose of a nondepolarizing agent four times higher than the ED95 dose can be used.
e Maintenance bolus doses to be given when the TOF count reaches 2-3 are generally 20%-25% of the initial bolus dose.
f Continuous infusion should be initiated only after early evidence of spontaneous recovery from the initial bolus dose.
a Histamine release is dose and rate dependent and, therefore, less pronounced if drugs are injected slowly.
III. NEUROMUSCULAR BLOCKADE
A. Depolarizing Blockade
Succinylcholine (SCh), the only depolarizing NMBD, is composed of two ACh molecules linked together via an acetyl moiety. SCh binds to the α-subunits of the nicotinic AChR leading to depolarization of the postjunctional membrane. Because SCh is not degraded by AChE as rapidly as ACh, it persistently depolarizes the motor endplate, leading to inactivation of the voltage-gated sodium channels in the perijunctional zone that are necessary for propagation of the depolarization. Induction doses of SCh produce a rapid onset (about 1 minute) of a transient agonist effect (e.g., muscle twitch) followed by skeletal muscle paralysis lasting 4 to 6 minutes. These characteristics make SCh a common choice for facilitating rapid tracheal intubation.
1. SCh effect terminates when the drug diffuses away from the AChRs and is rapidly hydrolyzed by plasma cholinesterase (produced in the liver and also referred to as pseudocholinesterase) to succinylmonocholine and then, more slowly, to succinic acid and choline. This enzyme is not the same as AChE and is not found in the synaptic cleft. However, inhibitors of AChE affect both enzymes to different degrees.
2. Side effects of SCh are related to its agonist effects at both the nicotinic and muscarinic AChRs.
a. Myalgia is common postoperatively, especially in the muscles of the abdomen, back, and neck. It is attributed to muscle fasciculations and observed more frequently in females and younger patients after minor surgical procedures.
b. Cardiac dysrhythmias. SCh has no direct effect on the myocardium. However, ganglionic stimulation may increase heart rate and blood pressure in adults. Alternatively, SCh may stimulate muscarinic receptors at the sinus node, producing sinus bradycardia, a junctional rhythm, or even asystole, particularly in children and following repeated exposure within a short time interval (i.e., 5 minutes) in adults. Pretreatment of children with intravenous (IV) atropine immediately before SCh reduces the occurrence of bradyarrhythmias.
c. SCh depolarization exaggerates the usual transmembrane ionic flux and normally induces elevation of serum potassium by 0.5 to 1.0 mEq/L. However, life-threatening hyperkalemia and cardiovascular collapse may occur in patients with major burns, massive tissue injuries, extensive denervation of skeletal muscle, or upper motor neuron diseases. This effect is attributed to a proliferation of extrajunctional AChRs or damaged muscle membranes and a massive release of potassium upon stimulation. In patients with burns, the period of greatest risk is from 2 weeks to 6 months after the burn has been sustained. However, it is recommended to avoid SCh after the first 24 hours and for 2 years from the time of the injury. Patients with mild elevations of potassium related to renal failure may usually safely receive SCh.
d. A transient increase in intraocular pressure occurs 2 to 4 minutes following SCh, presumably due to contractions of the extraocular muscles with associated compression of the globe or cycloplegia causing obstruction of aqueous outflow via the trabecular meshwork. However, the use of SCh in open eye injuries is still acceptable for rapid sequence inductions (see Chapter 26).
e. Increased intragastric pressure results from fasciculations of abdominal muscles. The pressure increase (averaging 15 to 20 mm Hg in an adult) is counterbalanced by an even greater increase in the lower esophageal sphincter tone.
f. SCh produces a mild transient increase in intracranial pressure (see Chapter 25).
Only gold members can continue reading. Log In or Register to continue