Fig. 14.1
CT scan: a Pipkin II fracture of the left femoral head with posterior dislocation. Pipkin II fracture of the right femoral head without dislocation

Fig. 14.2
Shows a pre-oppelvis x-ray
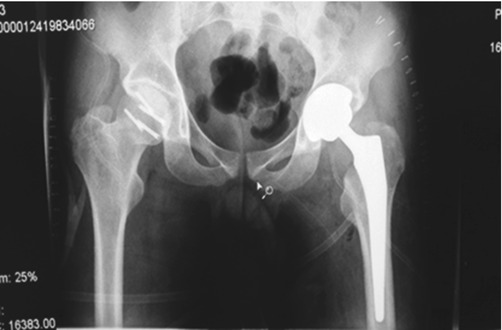
Fig. 14.3
Shows the post-op pelvic X-ray ORIF right femoral head THR left hip

Fig. 14.4
Shows the ORIF left femur

Fig. 14.5
ORIF right tibia

Fig. 14.6
Shows the ORIF left tibia
14.4 Diagnosis
- 1.
S/P high-energy polytrauma patient. S/P ORIF plating left femur and both tibia.
- 2.
Fracture dislocation of the left hip (Pipkin II).
- 3.
Fracture of the femoral head right hip (Pipkin II).
14.5 Surgical Management
On the day following his admission, the patient was taken to the operating room. Following the administration of general anesthesia, the right hip was addressed. A lateral approach (Hardinge) was used: the anterior capsule was opened, the joint was explored, and the femoral head fracture was reduced and fixated by headless screws. Anatomic reduction and stable fixation were achieved and confirmed by fluoroscopy. The stability of the joint was also confirmed.
Next, the patient was turned on his right side. A posterior (Kocher-Langenbeck) approach for the left hip was applied. The defect of the femoral head was great; the fragments were far too small and could not be fixated. The joint was replaced by cementless prosthesis with ceramic liner and head (Fig. 14.5).
14.6 Postoperative Management
On the second postoperative day, the patient was mobilized out of the bed with the aid of gutter crutches, full weight bearing on his left leg, and non-weight bearing on his right leg. One week postoperatively, the patient was discharged, returning to his country.
14.7 Discussion
Fracture of the femoral head with hip dislocations occurs as a result of a high-velocity injury frequently associated with multiple organ damage [2]. The mechanism of injury for femoral head fracture is traumatic dislocation of the hip. Shear forces against the femoral head as it exits the contained acetabulum are thought to cause the femoral head fracture. Due to the inherent stability of the hip joint, significant force is required to disrupt the posterior hip capsule, and more may be required to add a shearing injury and produce a femoral head fracture as the head is pushed against the posterior rim of the acetabulum [4, 6], most often due to motor vehicle collisions, fall from a height, motor vehicle-pedestrian accidents, and sports injuries. It is extremely rare that fractures of the hip should include both joints, left and right, and long bones. The combination of femoral shaft fracture and hip dislocation was first reported by Sir Astley Cooper in 1923—Helal and Skevis speculated that this injury is the result of two forces; the hip joint dislocated by axial impaction, and the femoral shaft fracture occurs after a direct blow to the thigh [7]. The incidence of long-term complications such as avascular necrosis (AVN) following posterior hip dislocation is about 13% and increases to 18% in the dislocations associated with femoral head fracture [6]. The rate of AVN may be affected by the time frame in which the femoral head remains dislocated [1, 4, 8].
Related posts:
 Things Aren’t Always What They Seem: The Case of Hala
Things Aren’t Always What They Seem: The Case of Hala
 Pelvic Injury
Pelvic Injury
 Multiple Malformations Embryo in a Syrian Pregnant Patient
Mediastinal Masses
Multiple Malformations Embryo in a Syrian Pregnant Patient
Mediastinal Masses
 Nonconventional Management of Bleeding Dysgerminoma in Adolescent Syrian Female
Nonconventional Management of Bleeding Dysgerminoma in Adolescent Syrian Female
 Acute Shortening and Angulation for Limb Salvage in Pediatric Patient After High-Energy Blast Injury
Acute Shortening and Angulation for Limb Salvage in Pediatric Patient After High-Energy Blast Injury
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


