CHAPTER 147
Nail Root Dislocation
Presentation
The patient has caught his finger in a car door or dropped a heavy object on his exposed toe, causing a painful deformity. The base of the nail will be found resting above the eponychium instead of in its normal anatomic position beneath. The cuticular line that had joined the eponychium at the nail fold will remain attached to the nail at its original position (Figures 147-1 to 147-3).
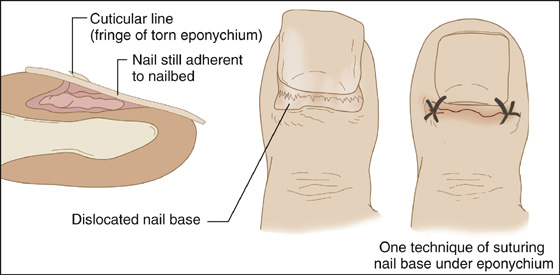
Figure 147-1 Dislocated nail root.

Figure 147-2 The subtle appearance of a dislocated nail root can be inadvertently overlooked by the clinician.

Figure 147-3 Appearance of the same toenail as shown in Figure 147-2 after a thorough cleansing, reinsertion of the nail root under the eponychium, and being sutured in place.
What To Do:
 Perform a thorough evaluation to ensure that neurovascular status is intact.
Perform a thorough evaluation to ensure that neurovascular status is intact.
 Obtain a radiograph to rule out an underlying fracture (which may require reduction as well as protective splinting).
Obtain a radiograph to rule out an underlying fracture (which may require reduction as well as protective splinting).
 Anesthetize the area using a digital block (see Appendix B).
Anesthetize the area using a digital block (see Appendix B).
 Lift the base of the nail off the eponychium and thoroughly cleanse and inspect the nail bed. Minimally débride loose cuticular tissue, and test for a possible avulsion of the extensor tendon (see Chapter 109).
Lift the base of the nail off the eponychium and thoroughly cleanse and inspect the nail bed. Minimally débride loose cuticular tissue, and test for a possible avulsion of the extensor tendon (see Chapter 109).
 If there are significant nail bed lacerations, the entire nail will need to be removed and lacerations repaired using a fine absorbable suture, such as 6-0 Vicryl or chromic gut (see Chapter 146). Just replacing the nail root into its normal position will correct most small and simple nail bed lacerations.
If there are significant nail bed lacerations, the entire nail will need to be removed and lacerations repaired using a fine absorbable suture, such as 6-0 Vicryl or chromic gut (see Chapter 146). Just replacing the nail root into its normal position will correct most small and simple nail bed lacerations.
 Using a hemostat, reinsert the root of the nail under the eponychium.
Using a hemostat, reinsert the root of the nail under the eponychium.
 Reduce any underlying angulated fractures by grabbing the distal phalanx and firmly bending it back into normal alignment. (This will help to stabilize and hold the nail root under the eponychium.) Unstable fractures may require fixations and consultation with a specialist.
Reduce any underlying angulated fractures by grabbing the distal phalanx and firmly bending it back into normal alignment. (This will help to stabilize and hold the nail root under the eponychium.) Unstable fractures may require fixations and consultation with a specialist.
 If the nail still tends to drift out from under the eponychium, it can be sutured in place using two 4-0 or 5-0 nylon or Prolene stitches in the proximal corners (see Figure 147-1).
If the nail still tends to drift out from under the eponychium, it can be sutured in place using two 4-0 or 5-0 nylon or Prolene stitches in the proximal corners (see Figure 147-1).
 Any nonabsorbable sutures should be removed after 1 week.
Any nonabsorbable sutures should be removed after 1 week.
 Cover the area with a fingertip dressing (see Appendix C), and splint any underlying fracture (see Chapter 111).
Cover the area with a fingertip dressing (see Appendix C), and splint any underlying fracture (see Chapter 111).
 Provide tetanus prophylaxis (see Appendix H).
Provide tetanus prophylaxis (see Appendix H).
 Follow-up should be provided in 3 to 5 days. Patients should be advised to leave the dressing and splint (if applicable) in place until his or her follow-up evaluation. If the dressing becomes wet or soiled, the patient should return immediately for redressing of the wound.
Follow-up should be provided in 3 to 5 days. Patients should be advised to leave the dressing and splint (if applicable) in place until his or her follow-up evaluation. If the dressing becomes wet or soiled, the patient should return immediately for redressing of the wound. Instruct patients to return immediately if there is increasing pain or any other sign of infection (redness, swelling, purulent drainage, or red streaking). The patient should be advised that it is normal to have blood continue to ooze from beneath nail in the first 1 to 2 days following his or her injury.
Instruct patients to return immediately if there is increasing pain or any other sign of infection (redness, swelling, purulent drainage, or red streaking). The patient should be advised that it is normal to have blood continue to ooze from beneath nail in the first 1 to 2 days following his or her injury.
 Prescribe appropriate pain management, including Tylenol and anti-inflammatories such as ibuprofen, as well as narcotic medications if indicated. Instruct the patient to keep the extremity elevated above the level of the heart as much as possible for further comfort.
Prescribe appropriate pain management, including Tylenol and anti-inflammatories such as ibuprofen, as well as narcotic medications if indicated. Instruct the patient to keep the extremity elevated above the level of the heart as much as possible for further comfort.
 Prophylactic antibiotics are not routinely required, even with associated fractures of the distal phalanx, except in immunocompromised patients. Significantly contaminated wounds should receive 3 to 5 days of cephalexin (Keflex), 500 mg qid.
Prophylactic antibiotics are not routinely required, even with associated fractures of the distal phalanx, except in immunocompromised patients. Significantly contaminated wounds should receive 3 to 5 days of cephalexin (Keflex), 500 mg qid.
What Not To Do:
 Do not ignore the nail root dislocation and simply provide a fingertip dressing. This is likely to lead to continued bleeding or to a later infection, because tissue planes have not been replaced into their natural anatomic position.
Do not ignore the nail root dislocation and simply provide a fingertip dressing. This is likely to lead to continued bleeding or to a later infection, because tissue planes have not been replaced into their natural anatomic position.
 Do not débride any portion of the nail root, nail bed, sterile matrix, or germinal matrix.
Do not débride any portion of the nail root, nail bed, sterile matrix, or germinal matrix.
 Do not neglect to thoroughly irrigate the injury site to minimize the risks of infection, as well as to meticulously repair the nail bed to prevent complications and to maximize cosmetic appearances.
Do not neglect to thoroughly irrigate the injury site to minimize the risks of infection, as well as to meticulously repair the nail bed to prevent complications and to maximize cosmetic appearances.
Discussion
The germinal matrix lies protected under the eponychium, forming the area from which the nail is produced. Growth takes place in the nail root, or lunula. The lunula is the pale crescent-shaped structure under the proximal portion of the nail.
Because the nail is not as firmly attached at the lunula and root as it is to the distal nail bed, impact injuries can avulse only the base (nail root), leaving the nail lying on top of the eponychium.
It may be surprising that this injury is often missed, but at first glance, a dislocated nail can appear to be in place, and without careful inspection, a patient can return from radiology with negative radiographs and be treated as if he only had an abrasion or a contusion. The attachment of the cuticle from the nail fold of the eponychium to the base of the nail forms a constant landmark on the nail. If any nail is showing proximal to this landmark, it indicates that the nail is not in its normal position beneath the eponychium.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


