CHAPTER 146
Nail Bed Laceration
Presentation
The patient has either cut into his nail with a sharp edge or crushed his finger (commonly in a door). With shearing forces, the nail may be avulsed from the nail bed to varying degrees, and there may be an underlying bony injury.
What To Do:
 Provide appropriate tetanus prophylaxis (see Appendix H).
Provide appropriate tetanus prophylaxis (see Appendix H).
 Obtain radiographs of any crush injury. Distal tuft fractures are common with these injuries.
Obtain radiographs of any crush injury. Distal tuft fractures are common with these injuries.
 Complex crush injuries or injuries resulting in significant tissue loss or deformity require specialty consultation with a hand surgeon.
Complex crush injuries or injuries resulting in significant tissue loss or deformity require specialty consultation with a hand surgeon.
 A small, stable laceration through the nail, with minimal wound separation, can simply be cleansed and sealed with tissue adhesive (Dermabond).
A small, stable laceration through the nail, with minimal wound separation, can simply be cleansed and sealed with tissue adhesive (Dermabond).
 With a larger or more complicated laceration through the nail, remove the entire nail to allow suturing of the nail as follows:
With a larger or more complicated laceration through the nail, remove the entire nail to allow suturing of the nail as follows:
 Perform a digital block for anesthesia (see Appendix B).
Perform a digital block for anesthesia (see Appendix B).
 A bloodless field may need to be established using a finger tourniquet.
A bloodless field may need to be established using a finger tourniquet.
 Use a straight hemostat or periosteal elevator to separate the nail from the nail bed (Figure 146-1). Keep instrument pointed toward the nail plate and not toward the nail bed, to prevent further injury.
Use a straight hemostat or periosteal elevator to separate the nail from the nail bed (Figure 146-1). Keep instrument pointed toward the nail plate and not toward the nail bed, to prevent further injury.
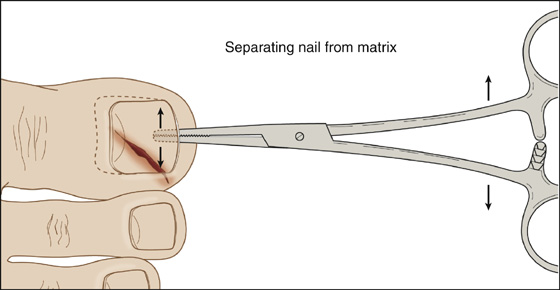
Figure 146-1 Separate nail from nail bed using a straight hemostat.
 Cleanse the wound thoroughly with saline.
Cleanse the wound thoroughly with saline.
 Suture with a fine absorbable material (6-0 or 7-0 Vicryl or Dexon) (Figure 146-2).
Suture with a fine absorbable material (6-0 or 7-0 Vicryl or Dexon) (Figure 146-2).
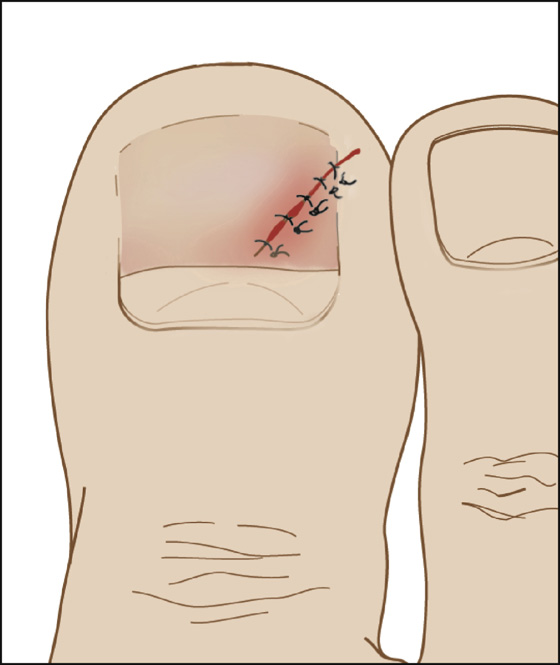
Figure 146-2 The nail bed can be repaired after it has been fully exposed.
 Replace the nail back into its normal anatomic position, as noted below.
Replace the nail back into its normal anatomic position, as noted below.
 When a crush injury results in open hemorrhage from under the fingernail, manage as follows:
When a crush injury results in open hemorrhage from under the fingernail, manage as follows:
 Perform a digital block for anesthesia (see Appendix B).
Perform a digital block for anesthesia (see Appendix B).
 The nail must then be completely elevated to allow proper inspection of the damaged nail bed.
The nail must then be completely elevated to allow proper inspection of the damaged nail bed.
 A bloodless field may need to be established with a finger tourniquet to help visualization.
A bloodless field may need to be established with a finger tourniquet to help visualization.
 Angulated fractures need to be reduced (see Chapter 111).
Angulated fractures need to be reduced (see Chapter 111).
 Large nail bed lacerations should be sutured with a fine absorbable suture (6-0 or 7-0 Vicryl or Dexon). Small lacerations with minimal wound edge separation do not require suturing.
Large nail bed lacerations should be sutured with a fine absorbable suture (6-0 or 7-0 Vicryl or Dexon). Small lacerations with minimal wound edge separation do not require suturing.
 An intact nail should be cleaned and reinserted for protection and proper tissue alignment, or an alternative nail bed dressing can be applied (see Chapter 138).
An intact nail should be cleaned and reinserted for protection and proper tissue alignment, or an alternative nail bed dressing can be applied (see Chapter 138).
 Tissue adhesive can be used to bond the nail to the nail bed and seal open spaces or defects in the nail (see Chapter 138). Cover with an appropriate fingertip dressing.
Tissue adhesive can be used to bond the nail to the nail bed and seal open spaces or defects in the nail (see Chapter 138). Cover with an appropriate fingertip dressing.
 Inform the patient that a new nail will slowly push off the replaced nail or artificial stent.
Inform the patient that a new nail will slowly push off the replaced nail or artificial stent.
What Not To Do:
 Do not use nonabsorbable sutures to repair the nail bed. The patient will be put through unnecessary suffering when the sutures are removed.
Do not use nonabsorbable sutures to repair the nail bed. The patient will be put through unnecessary suffering when the sutures are removed.
 Do not place a dressing that requires removal onto an exposed nail bed. Any such dressing will adhere tenaciously to the nail bed and will be extremely painful to remove (even after a short period of time).
Do not place a dressing that requires removal onto an exposed nail bed. Any such dressing will adhere tenaciously to the nail bed and will be extremely painful to remove (even after a short period of time).
Discussion
The objective of a nail bed repair is to provide a flat, smooth surface on which the new nail will grow. It is crucial that the provider is attentive while addressing these injuries, because mismanagement can lead to further complications. If a wound is inadequately repaired or if a wound is allowed to heal by secondary intention, additional scar tissue may cause the nail to split or become nonadherent.
It is also necessary to provide separation of the eponychium from the germinal matrix to prevent potential adhesions from forming. Replacement of the original nail into its normal anatomic position, with the nail root under the eponychium, is the best method of preserving future nail integrity. When the nail has been severely damaged or is missing, an artificial stent can be provided (see Chapter 138).
Significant nail bed injuries can be hidden by hemorrhage and a partially avulsed overlying nail. These injuries must be repaired to help prevent future deformity of the nail (Figure 146-3). Surgical consultation should be obtained when nail bed lacerations involve the germinal matrix under the base of the nail.
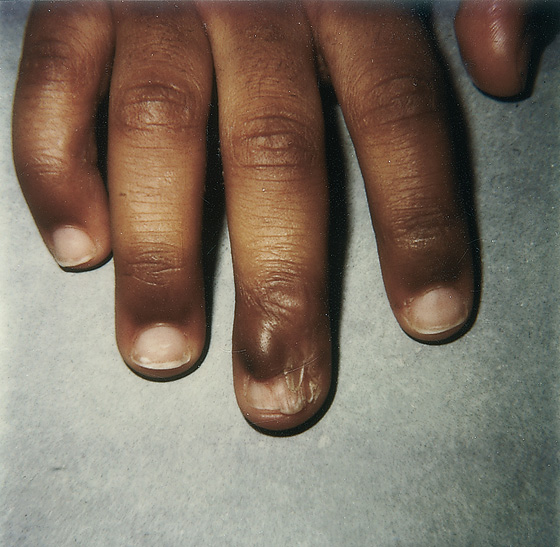
Figure 146-3 Improper nail bed repair will increase the risk for future fingernail or toenail deformity.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


