MUSCULOSKELETAL INJURIES
OVERUSE SYNDROMES
Carpal Tunnel Syndrome
Carpal tunnel syndrome is caused by elevated pressure in the “carpal tunnel,” which is a space at the base of the wrist through which pass nine tendons that flex (bend toward the palm) the fingers, along with the median nerve. It can be caused for a number of reasons, which include forceful, repetitive use of the wrist. The pressure causes the median nerve to have diminished function, which leads to the signs and symptoms. These include pain, numbness, tingling, and/or burning sensation on the palm side of the thumb, index finger, middle finger, and thumb side of the fourth finger. The “pinkie” side of the fourth finger and fifth finger are spared, as they are serviced by the ulnar nerve, which lies outside the carpal tunnel. Treatment is to avoid the offending activity and to splint the wrist in a “neutral” position of function (see page 73), both night and day if possible. A nonsteroidal antiinflammatory drug may be helpful. If the case is severe, a physician may prescribe oral steroids or inject steroids into the carpal tunnel. Medical evidence does not support the use of vitamin B6. If carpal tunnel syndrome persists and the victim shows loss of nerve function or muscle wasting at the base of the thumb, surgery may be advised to decrease the pressure.
Shin Splints
Shin splints is the term used to describe a painful disorder generated by excessive walking, running, or hiking. The sufferer has irritated the thin membrane that connects his two lower leg bones along the longitudinal axes where the membrane attaches to the bones. With every footstep, there is further irritation of the membrane, so that it can become impossible to walk rapidly. The victim should attempt to curtail running or vigorous walking activity, and may benefit from the administration of aspirin or a nonsteroidal antiinflammatory drug (such as ibuprofen or naproxen). A shoe that is well cushioned (particularly its ball and heel) is very important for prevention and recovery. More complex orthotics may be required.
Plantar Fasciitis
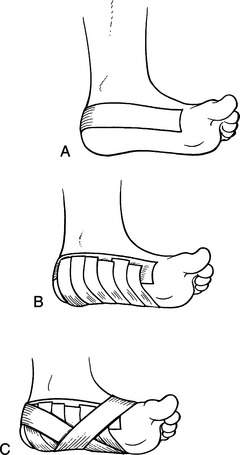
If the victim must continue to walk on the painful foot, it can be taped to provide arch support; this can do much to reduce pain. It is accomplished as follows: Apply a thin layer of benzoin or spray tape adhesive onto the bottom of the foot. Fix an anchor strip of ¾ in (1.9 cm) adhesive tape in a U shape around the heel from just under the malleoli (prominences of the ankle) up to just behind the level of the “knuckles” of the toes (Figure 169, A). Next, lay fairly tight cross-strips of ½ in (1.3 cm) tape across the bottom of the foot, with their ends torn to lay on the anchor strip (Figure 169, B). This creates a “sling” of tape under the foot for support. Finally, apply another U-shaped piece of tape around the heel that crosses under the center of the arch and locks down the crosspieces (Figure 169, C).
Torn Muscle
A torn muscle (“pulled” muscle) is recognized as sudden pain in a muscle group associated with a particular vigorous exertion, such as sprinting or lifting a heavy object. Depending on the severity of the injury, there may be associated bruising, swelling, loss of mobility, and/or weakness. For instance, a small tear in the deltoid muscle of the shoulder may cause minor discomfort on lifting the arm over the head, while a complete separation of the quadriceps group in the anterior thigh will cause inability to straighten the leg at the knee, extreme local pain, blue discoloration of the knee, and a defect in the shape of the muscles above the knee that is easily felt and seen.
Minor muscle injuries should be treated in the first 24 hours with immobilization, the application of cold (insulated ice packs or chemical cold packs, for example; do not apply ice directly to the skin) for 30 to 45 minutes every 2 to 3 hours, and elevation. After 48 to 72 hours, the application of heat (warm water or a heating pad, not ointments) and gentle movement should be started. If a significant injury is suspected (for example, complete tear of the biceps muscle or quadriceps muscle group), the injury should be immobilized as for a fracture (see page 74) and the victim transported to a physician.


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


