CHAPTER 11 Monitoring
Monitoring
Most studies that have determined the rate of cardiac arrests resulting from anesthesia have found a threefold to fivefold greater risk among children than adults (Graff et al., 1964; Keenan and Boyan, 1985). In children younger than 1 year, the incidence increases to 9.2 to 17 per 10,000 anesthesias, or 10 times the adult incidence (Olsson and Hallen, 1988; Cohen et al., 1990). Factors contributing to cardiac arrests in anesthetized children are likely to be related to the cardiovascular or respiratory system (Salem et al., 1975). Flick and others (2007) have reviewed cardiac arrest data at the Mayo Clinic. The incidences of cardiac arrest and mortality during noncardiac procedures were 2.9:10,000 and 1.6:10,000, respectively. However, the incidence of cardiac arrest in children undergoing cardiac operations was 127:10,000. The incidence of other serious complications is also greater for infants than for adults in the operating room (Tiret et al., 1988) and in the postanesthesia care unit (PACU) (Cohen et al., 1990). These data indicate that children are a high-risk population and should be monitored with particular attention to cardiovascular and respiratory variables.
Guidelines for the intraoperative monitoring of patients under anesthesia have been published by the American Society of Anesthesiologists (ASA) (2005) (see Box 10-1). These standards mandate the continuous presence of an anesthesiologist or a nurse anesthetist throughout the conduct of anesthesia and require continuous monitoring of oxygenation, electrocardiographic status, and adequacy of ventilation and circulation. The minimum standard for monitoring oxygenation includes an oxygen analyzer in the anesthesia breathing circuit, sufficient illumination to evaluate the patient’s color, and a quantitative method such as pulse oximetry, except under extenuating circumstances. Tracheal intubation must be verified by physical examination and the qualitative detection of carbon dioxide in the exhaled gas. Regardless of whether endotracheal intubation has been performed, continuous capnography is required unless it is invalidated by the nature of the patient, procedure, or equipment. Furthermore, quantitative monitoring of the volume of expired gas is strongly encouraged. The ASA also recommends monitoring of ventilation using observation of chest excursion and the reservoir breathing bag, as well as auscultation of breath sounds. When ventilation is controlled by a mechanical ventilator, there should be in continuous use a device that is capable of detecting disconnection of components of the breathing system, and the device must give an audible signal when its alarm threshold is exceeded.
Physical Examination
Observation
The anesthesiologist can gain a tremendous amount of information from observation alone. Anesthetic depth can be inferred from the rate and pattern of respiration, and airway obstruction can be detected by chest wall retractions or “seesaw” paradoxical motion. The skin and mucous membranes should be continually assessed to confirm adequate oxygenation, because a pulse oximeter reading can significantly lag behind other indices of hypoxemia when placed on an extremity (Reynolds et al., 1993), or it may not detect a pulse at all during intense vasoconstriction. In rare circumstances, pulse oximetry falsely indicates normal saturations during hypoxic conditions (Costarino et al., 1987).
Auscultation
Esophageal stethoscopes are contraindicated in patients with esophageal atresia or in those who have a disease process involving the proximal portion of the esophagus. They confer a rigid feel to the esophagus, which might be mistaken for the trachea (Schwartz and Downes, 1977). As a result, the esophageal stethoscope is relatively contraindicated in neck dissections where the trachea is a critical landmark, such as a tracheostomy.
Electrocardiography
In children, the normal heart rate varies with age (Table 11-1). The normal heart rate of the newborn ranges from 120 to 160 beats per minute, although lower rates (e.g., 70) are frequently observed during sleep, and higher rates (>200) are common during anxiety or pain. Heart rates tend to decrease with age and in parallel with decreases in oxygen consumption. In addition, many children have a noticeable variation in heart rate with respiration (i.e., sinus arrhythmia).
TABLE 11-1 Normal Resting Heart Rates of Infants and Children
| Age | Heart Rate (beats/min) | |
|---|---|---|
| Mean | Range (±2 SD) | |
| 0 to 24 hr | 119 | 94 to 145 |
| 1 to 7 days | 133 | 100 to 175 |
| 8 to 30 days | 163 | 115 to 190 |
| 1 to 3 mo | 152 | 124 to 190 |
| 3 to 12 mo | 140 | 111 to 179 |
| 1 to 3 yr | 126 | 98 to 163 |
| 3 to 5 yr | 98 | 65 to 132 |
| 5 to 8 yr | 96 | 70 to 115 |
| 8 to 16 yr | 77 | 55 to 105 |
Modified from Liebman J, Plonsey R, Gillette PC, editors: Pediatric electrocardiography, Baltimore, Md, 1982, Williams & Wilkins.
Systemic Arterial Pressure
Noninvasive Measurement
Blood pressure is easily measured noninvasively in children and small infants using oscillotonometry. In children, oscillometric measurements of systolic arterial pressure (Bruner et al., 1981; Friesen and Lichtor, 1981) and mean arterial pressure (Kimble et al., 1981) usually correlate well with the Riva Rocci mercury column method, as well as with direct arterial pressure measurement, but oscillometric measurements tend to underestimate the diastolic component. During routine uncomplicated cases, measurement of blood pressure should be performed every 3 to 5 minutes while the child is anesthetized—determinations that are too frequent can result in limb ischemia. The blood pressure cuff is most commonly placed on the upper arm but can be placed on the forearm, thigh, or calf. There is inconsistent correlation of measurements obtained between the upper and lower limbs.
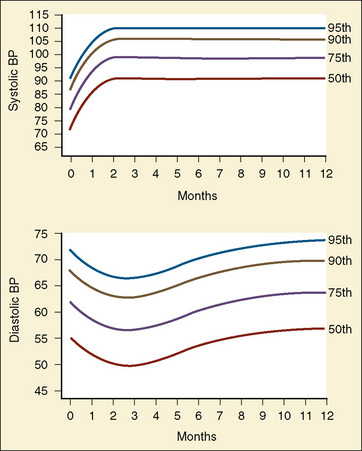
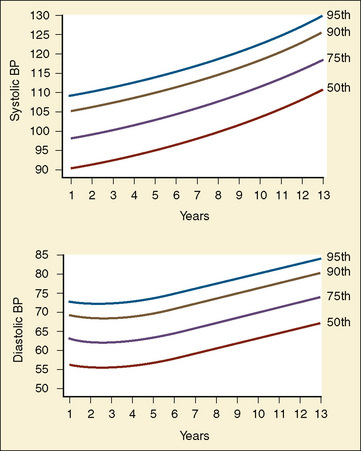
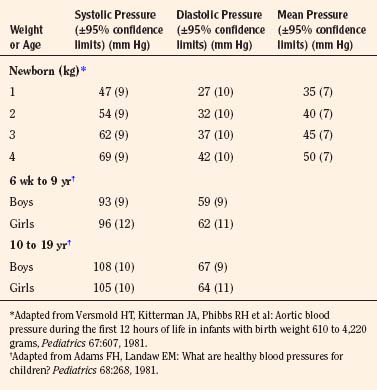
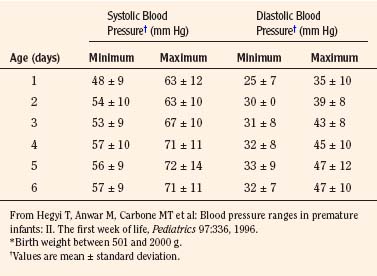
The width of the blood pressure cuff should cover approximately two thirds of the total length of the upper arm (or other extremity portion to which it is applied). A cuff that is too small or too narrow incompletely occludes the artery, resulting in the premature return of detectable flow and hence falsely increasing the pressure measurement (Park et al., 1976; Kimble et al., 1981). The error can be as great as 30 mm Hg. A cuff that is too wide can dampen the arterial wave and result in a falsely low pressure, but the magnitude of this error is small (Kimble et al., 1981). Blood pressure increases gradually throughout childhood (Figs. 11-1 and 11-2) and depends on the height of the child: taller children demonstrate a higher blood pressure (Table 11-2). Blood pressure ranges in premature infants have been defined (Table 11-3) and vary depending on the health status of the infant and mother.
Direct Measurement
There are no absolute contraindications to placing an arterial catheter, but a risk-benefit analysis should be performed in patients with a hypercoagulable state or bleeding disorder. The radial artery is a favored site for arterial cannulation because the vessel is superficial and easily accessible. Other anatomic sites frequently used are the ulnar, dorsalis pedis, posterior tibial, and femoral arteries. The axillary artery has gained favor because of increased collateral blood flow compared with the brachial or femoral artery (Lawless and Orr, 1989; Cantwell et al., 1990; Greenwald et al., 1990; Piotrowski and Kawczynski, 1995). In general, the brachial artery should be avoided because of the risk for median nerve damage and poor collateral flow around the elbow. Umbilical vessels are an alternative site for cannulating the aorta and inferior vena cava in neonates. In determining a site, one needs to consider the history of that vessel (i.e., whether it has been cannulated before), its collateral flow, the experience of the person inserting the catheter, and special physiologic issues (e.g., whether it arises on an aortic root proximal to the ductus arteriosus) or surgical issues (e.g., whether it arises from a vessel likely to be clamped or sacrificed during the procedure). Cannulation of vessels with good collateral flow, such as the arch vessels of the wrist or foot, may reduce the risk for ischemic tissue damage distal to the catheter.
As the largest superficial vessel, the femoral artery can be cannulated most predictably in situations when intense peripheral vasoconstriction may accompany low cardiac output and blood pressure. In less dire circumstances, the selection of a vessel may reflect a variety of anatomic and physiologic characteristics exhibited by certain vessels. The pedal vessels exhibit pressure wave amplification that results in pressure determinations exceeding aortic values by as much as 30% (Park et al., 1983).
A Doppler flow transducer is occasionally useful to locate an artery that is difficult to palpate. Surgical cutdown may be the preferred option when percutaneous placement is likely to be difficult or has failed. Indwelling arterial catheters are associated with several possible complications. Proximal emboli, distal ischemia, arterial thrombosis, and infection are common to all sites. Thrombosis of the radial artery is generally temporary, although it is more likely to persist after a cutdown (Miyasaka et al., 1976). Although small flush volumes (0.3 mL) in radial arterial catheters can be detected in the aortic arch vessels, cerebral infarcts have not been reported (Edmonds et al., 1980). The tip of an umbilical artery catheter should be placed in either a high (above the diaphragm) or a low (below L3) position to avoid direct flushing into the renal arteries. Despite these precautions, as many as 10% of neonates exhibit hypertension as a late complication attributed to umbilical artery catheterization (Bauer et al., 1975; Plumer et al., 1976; Horgan et al., 1987). Minor complications of umbilical artery monitoring include vasospasm of the lower extremity vessels, which are more common with low tip placement. Major complications (e.g., necrotizing enterocolitis, renal artery thrombosis) occur independent of location (Mokrohisky et al., 1978; Umbilical Artery Catheter Trial Study Group, 1992). The rarity of clinical complications is remarkable given that the incidence of aortic thrombosis on removal of umbilical artery catheters approaches 95% in some series (Neal et al., 1972), although most series define the incidence at 12% to 31% of neonates (Symansky and Fox, 1972; Horgan et al., 1987; Seibert et al., 1987).
Systolic Pressure Variation
Systolic pressure variation is a noninvasive way to determine volume status and fluid responsiveness. It is defined as the difference between the maximal and minimal values of systolic blood pressure during a positive pressure breath. Initially during a positive pressure breath, there is a transient increase in systolic blood pressure (delta up) followed within four or five beats by a decrease in systolic blood pressure (delta down). Increases in intrathoracic pressure during positive pressure ventilation cause a decrease in systolic blood pressure because of decreased preload to the right ventricle, increased afterload to the right ventricle, and decreased afterload to the left ventricle. This decrease is greater during hypovolemia. Systolic pressure changes in response to respiratory variation have been used to determine hypovolemia (Greilich and Johnston, 2007).

where ΔPP% is respiratory change in pulse pressure (mm Hg).
Michard and others (1999) demonstrated a strong relationship in adult ventilated patients between pulse pressure changes and cardiac output. Patients with pulse pressure changes (ΔPP) that are greater than 10% may be fluid responsive and benefit from the administration of intravenous fluids.
Changes in the pulse oximetry waveform (plethysmographic waveform amplitude) have been shown to predict fluid responsiveness (Pizov et al., 2010). Bedside use of this variable is challenging. The “pleth variability index” (Masimo Corp., Irvine, CA) automatically calculates the waveform amplitude variation and may predict fluid responsiveness noninvasively (Cannesson et al., 2008a, 2008b).
Central Venous Pressure
Catheters of various sizes (2.5 to 10 French), lengths, and composition are available for pediatric applications (Cook Critical Care, Bloomington, IN, and other companies). Selection is based on the size of the patient (Andropoulos et al., 2001) and the purpose of the catheter. The composition of the catheter depends on its intended use. Teflon is fairly resistant to thrombus formation, but concerns about perforation by catheters have prompted the development of softer catheter materials, especially for long-term use (e.g., Silastic and polyurethane). The catheters are generally inserted via the Seldinger technique, using landmarks that are similar to those used in adults.
There are no absolute contraindications to placing a central venous catheter, but each site has potential risks. All sites share the common complications of infection (site cellulitis, bacteremia), venous thrombosis with potential emboli, air embolism, catheter malfunction (occlusion, dislodgment, or fractures), dysrhythmias (when the catheter tip is in the heart), and bleeding. Universal precautions and sterile technique should be used when placing a central venous catheter. The risks involved in cannulating the internal jugular vein include carotid artery puncture, Horner’s syndrome, pneumothorax, and injury to the thoracic duct when the left internal jugular vein is cannulated. The high approach to the internal jugular vein, at the midpoint of the sternocleidomastoid muscle, results in comparable success with fewer complications than lower approaches (Coté et al., 1979). Two-dimensional ultrasound scanning improves localization of the internal jugular vein and increases the success rate of central venous cannulation in adults and children (Verghese et al., 2002; Hind et al., 2003). Using this device, Alderson and others (1993) reported an 18% prevalence of anatomic variations in children younger than 6 years that would preclude or significantly hinder the successful cannulation of the internal jugular vein using anatomic landmarks alone. In addition, Hong and colleagues (2010) reported that rotating the head away from the neutral position increases the degree of carotid artery and internal jugular vein overlap, and decreases the incidence of lateral positioning of the internal jugular vein to the carotid artery.
Mixed Venous Oxygenation and Monitoring
 ), cardiac output, hemoglobin, and arterial oxygen saturation.
), cardiac output, hemoglobin, and arterial oxygen saturation. (hypothermia, anesthesia) or an increase in oxygen delivery (increased hemoglobin, increased cardiac output, increased Pao2, increased Sao2). Mixed venous oxygenation is used to assess the balance between oxygen delivery and oxygen consumption for patients in the operating room and intensive care unit. It is a global index of tissue oxygenation.
(hypothermia, anesthesia) or an increase in oxygen delivery (increased hemoglobin, increased cardiac output, increased Pao2, increased Sao2). Mixed venous oxygenation is used to assess the balance between oxygen delivery and oxygen consumption for patients in the operating room and intensive care unit. It is a global index of tissue oxygenation.Dueck and coworkers (2005) found a significant variation between central venous saturations and mixed venous saturations in the same patient, so individual values of Scvo2 cannot be substituted for Svo2 values. However, although the absolute values do not correlate, there is a correlation between the trends in Scvo2 values and in Svo2 values. Perez and colleagues (2009), in a retrospective pediatric study, identified a correlation between right atrial and mixed venous oxygen saturations. Scvo2 is used clinically in pediatric patients. Continuous monitoring of Scvo2 can be performed in neonates, infants, and children.
In infants, continuous monitoring of Scvo2 can be achieved with a fiberoptic probe. One type of fiberoptic probe is designed as a percutaneous catheter from CeVOX (Pulsion Medical Systems AG, Munich, Germany). This 2-F probe is 31 cm in length and measures central venous oxygen saturations using spectrophotometry. Muller and coworkers (2007) described placing the catheter percutaneously through a 16-gauge single-lumen catheter in the femoral or subclavian vein. There were only three patients in this study, so accurate correlation with central venous blood samples cannot be determined.
The Pediasat system (Edwards Life Sciences) has been described in infants and children having orthopedic, craniofacial, and cardiac surgery. It comes in four sizes (4.5 F, 5 cm; 4.5 F, 8 cm; 5.5 F, 8 cm; and 5.5 F, 15 cm) and provides continuous readings of central venous oxygen saturation. Liakapolous and colleagues (2007) and Ranucci and colleagues (2008) demonstrated good correlation between Scvo2 values from the Pediasat system when compared with co-oximetry values obtained from blood samples drawn from the distal port.
Pulmonary Artery Catheters
Since its introduction in 1970, indications for the use of the flow-directed balloon-tipped pulmonary artery (Swan-Ganz) catheter in pediatric patients have been slow to evolve. Although the validity and value of the data that these catheters generate remain controversial in pediatrics, the technical difficulties and complications associated with their use are significant. Pulmonary artery pressure measurement can help guide therapy in children with elevated or volatile pulmonary vascular resistance, but the interpretation of the flow data they generate is hindered by several factors. First, the desired cardiac output varies according to age, disease state, and other elements of management that alter metabolic demand in complex ways, thereby introducing significant uncertainty in assigning a target value. Second, the prevalence of intracardiac communications that permit shunting of blood causes discrepancies in pulmonary and systemic blood flow that may vary continuously and are difficult to quantify. Finally, despite several studies demonstrating reasonable accuracy when thermodilution is compared with other methods of flow determination, such as the Fick equation (Freed and Keane, 1978) and dye dilution (Colgan and Stewart, 1977), the precision of these determinations in small infants is low and has a 25% intersample variability. In patients with congenital heart malformations, for example, measurement errors are introduced by shunting and complex anatomy, and the risks of improper placement of the flow-directed pulmonary artery catheter are increased. Alternatively, directly placed pulmonary artery catheters can provide the necessary information regarding pulmonary vascular resistance and residual left-to-right shunts, and left atrial catheters reflect filling and diastolic function of the left ventricle after cardiac surgery.
Pulmonary artery catheters can be difficult to insert, especially in infants or in children with low cardiac output. They may be placed in any vein used for access to the central venous system, but the most reliable veins are the right internal jugular and the femoral. In infants and children smaller than 15 kg, it is technically difficult to place an introducer sheath in the neck vessels; the femoral veins are preferable. Multilumen catheters capable of thermodilution are available in two sizes, 5 and 7 F, with four options for the right atrium–to–pulmonary artery interluminal distance. Catheter recommendations are based on age (Table 11-4). The proper placement of these catheters can take a long time, and thus the assistance of fluoroscopy is recommended for infants and children less than 30 kg and for larger children who have a low cardiac output.
TABLE 11-4 Guidelines for Multilumen Pulmonary Artery Catheters for Infants and Children
| Age (yr) | Catheter Size (F) | CVP to Pulmonary Artery Port Distance (cm) |
| Newborn to 3 | 5 | 10 |
| 3 to 8 | 5 | 15 |
| 8 to 14 | 7 | 20 |
| >14 | 7 | 30 |
Cardiac output can be estimated in children through indicator dilution (e.g., thermodilution or dye dilution) and noninvasive techniques. Doppler determinations of aortic blood velocity can be used to quantify systemic flow if the angle of the incident ultrasound beam and the cross-sectional area of the aorta are reliably determined (Alverson et al., 1982). Transthoracic and transesophageal evaluations of Doppler cardiac output in children have proved to be less promising (Notterman et al., 1989; Muhiudeen et al., 1991). Thoracic bioimpedance, a method that estimates stroke volume on the basis of changes in thoracic impedance, has been applied to children as small as 3.6 kg. Although some correlation exists between bioimpedance and indicator dilution methods, reproducibility is poor (O’Connell et al., 1991). Further details and the complexities encountered in the measurement of cardiac output in children are beyond the scope of this chapter but have been reviewed previously (Tibby and Murdoch, 2002).
A noninvasive cardiac output monitor has been developed that determines cardiac output via the Fick principle for rebreathed CO2 (Respironics; Novametrix Medical Systems Inc., Wallingford, CT) (Capek and Roy, 1988). The noninvasive cardiac output monitor has been clinically validated in adults and is approved by the U.S. Food and Drug Administration (FDA) for use, but it requires tidal volumes of 200 mL or greater (Guzzi et al., 2003; Watt et al., 2004).
Transesophageal Echocardiography
The value of transesophageal echocardiography (TEE) for monitoring hemodynamics and to evaluate preoperative and postoperative cardiac anatomy has been appreciated from the time of its introduction to the operating room. In the infancy of TEE in the late 1970s, an M-mode transducer was passed into the esophagus, plotting the distance of structures from the transducer on the y-axis and time on the x-axis (Frazin et al., 1976). Although they provided valuable information, M-mode images were too limited alone. In 1982, Schlüter and colleagues (1982) described their experience using a transducer capable of two-dimensional images mounted on a gastroscope. The usefulness of the images obtained was readily apparent, and since that time technology has catapulted the field of TEE to the forefront of cardiovascular monitoring. Now, multiple companies (Phillips, Acuson/Siemens, General Electric) manufacture advanced TEE-specific probes capable of two- and three-dimensional imaging on top of the original M-mode. Doppler has also been incorporated, providing the examiner the ability to extrapolate vast amounts of information from their patients.
A modification of the Bernoulli equation allows an examiner to estimate pressure gradients using the measured velocities. Simplified, the change in pressure between two points is equal to four times the maximum velocity squared (Holen et al., 1977; Hatle et al., 1978). Using this principle, the stenosis of valves, severity of aortic coarctation, obstruction caused by muscle bundles or membranes, and a multitude of other clinical questions can be answered.
TEE has played a vital role in improving outcomes in pediatric patients with congenital heart disease. Typically, examinations are performed preoperatively to confirm anatomy, and postoperatively to assess repairs and evaluate function. One study looking at 865 consecutive examinations demonstrated alterations to surgical plans based on preoperative TEE examinations in 2% of patients. The same study found that 12% of patients had post-bypass examinations that led to surgical interventions. Many of these interventions saved patients from unnecessary revision operations and their associated morbidity. In addition to surgical interventions, medical management with drugs and fluids was affected in 20% of the examined patients (Bettex et al., 2003).
An earlier report found that pediatric patients leaving the operating room without residual defects seen on the echocardiographic examination had a risk for reoperation of 3%, versus 42% for those who were found to have residual defects (Ungerleider et al., 1989). This ability to detect problems early provides a significantly improved outcome and subsequently reduces costs, as the need for repeat operations is reduced (Randolph et al., 2002).
As evidence supporting the value of TEE in cardiac surgery has increased, recommendations for proper performance of the examination have matured. The American Society of Echocardiographers and the Society of Cardiovascular Anesthesiologists have developed guidelines for adult intraoperative TEE examinations to encourage complete examinations with standardized views and nomenclature so as to improve communication between various care providers (Shanewise et al., 1999). Discussion of the complete examinations is beyond the scope of this chapter, but some of the probe locations and angles are useful for obtaining basic information regarding a patient’s condition (Table 11-5). Similar guidelines have also been published to assist clinicians with the pediatric examination (Lai et al., 2006).
TABLE 11-5 Transesophageal Echocardiography Cross Sections
| Location | Angle (degrees) | Structures Visualized |
| Transgastric | 0-20 | Left and right ventricles, and both atrioventricular valves |
| 80-100 | Two-chamber view of left side | |
| 90-120 | Long axis of left side, including left ventricular outflow tract | |
| Midesophageal | 0-20 | Standard four-chamber view |
| 30-60 | Aortic valve on short axis, coronary arteries | |
| 60-90 | Right ventricular inflow and outflow tracts | |
| 80-110 | Bicaval view | |
| 120-160 | Long-axis view of aortic valve and left ventricular outflow tract | |
| Upper esophageal | 0 | Aortic arch on long axis |
| 90 | Aortic arch on short axis |
Modified from Shanewise JS, Cheung AT, Aronson S et al: ASE/SCA guidelines for performing a comprehensive intraoperative multiplane transesophageal echocardiography examination: recommendations of the American Society of Echocardiography Council for Intraoperative Echocardiography and the Society of Cardiovascular Anesthesiologists Task Force for Certification in Perioperative Transesophageal Echocardiography, J Am Soc Echocardiogr 12:884, 1999.
Although the benefits have been demonstrated, providers must also be aware of the complications associated with the TEE examination. Problems that may be encountered include damage to the oral cavity, esophagus, or stomach; compromised ventilation; inadvertent extubation; right main stem advancement; vascular compression; and arrhythmias. In light of these serious but rare events, caution should precede placement of the transesophageal probe (Stevenson, 1999). Contraindications to the TEE examination include an unrepaired tracheoesophageal fistula, esophageal web, and recent esophageal or gastric surgery. Failure to ascertain a history of such events may lead to significant damage or even perforation of the esophagus.
Temperature
Temperature monitoring is vital during pediatric anesthesia, as children may exhibit hypothermia or hyperthermia, both of which can have profound physiologic consequences (see Chapter 6, Thermoregulation).
Urine Output
Urine output often reflects intravascular volume status and cardiac output. Proper assessment of urine output requires recognition of the physiologic mechanisms that exert an affect on urine flow in children. During the first week of life, the glomerular filtration rate and renal plasma flow are only 25% of normal adult values (Arant, 1978). The neonatal kidney is limited in its ability to concentrate the urine (Simpson and Stephenson, 1993). By the end of the first week of life, the kidneys begin to reach absorption thresholds for sodium and glucose that approach adult levels.
Normal newborns produce between 0.5 and 4 mL urine/kg per hour in the first 3 hours of life (Strauss et al., 1981). Urine flow, which initially ranges from 15 to 60 mL/kg per day, reaches as much as 120 mL/kg per day by the end of the first week of life, with 90% of neonates producing 0.5 to 5 mL/kg per hour (Douglas, 1972; Guignard, 1982). In the neonate who is less than 1 week old, urine flow alone is not a sensitive index of changes in cardiac output or intravascular volume. The limited capacity of the neonatal kidneys to compensate for diminished or excessive intravascular volume demands more precise management of blood and fluid replacement in these infants. Beyond the neonatal period, a urine flow of 0.5 to 1 mL/kg per hour usually indicates adequate renal perfusion and function.
Noninvasive Respiratory Gas Monitoring
Carbon Dioxide
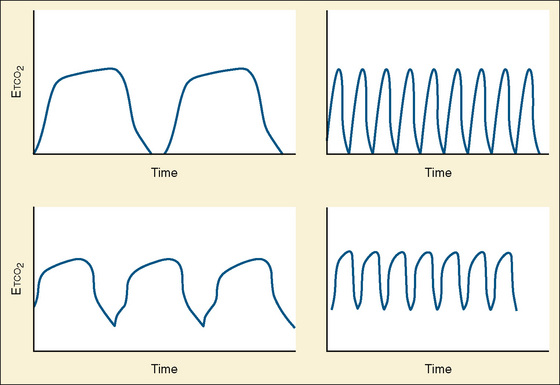
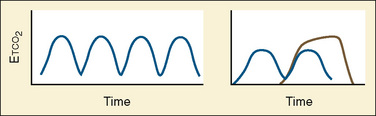
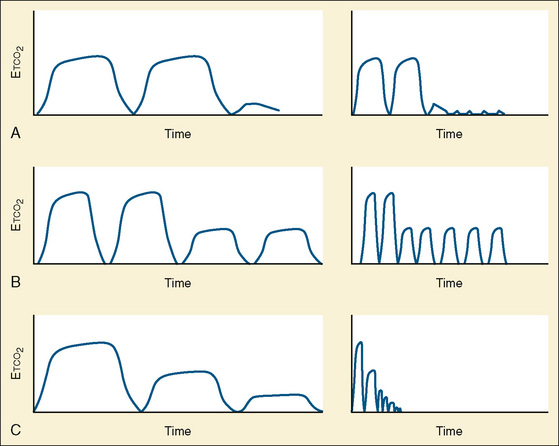
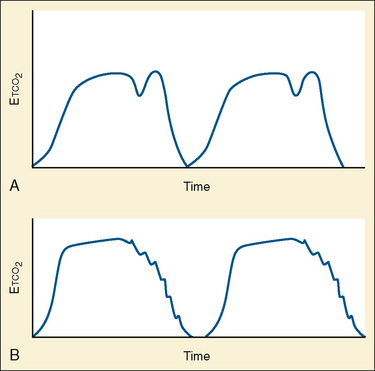
Capnometry is the instantaneous measurement of CO2 in the breathing circuit; it depicts this information in a continuous graphic display in which both the quality and the quantity of ventilation can be evaluated (Figs. 11-3 to 11-6).
Before 1998, capnography was considered a standard monitor by the ASA for confirming the initial placement and continuous presence of an endotracheal tube. This section of the ASA monitoring standards was updated in 1998 and states that capnography should be used to confirm adequate ventilation during general anesthesia with or without an endotracheal tube (during laryngeal mask airway, face mask, or natural-airway anesthesia). Specifically, these guidelines state, “Continual monitoring for the presence of expired carbon dioxide shall be performed unless invalidated by the nature of the patient, procedure or equipment…. Continual end-tidal carbon dioxide analysis, in use from the time of endotracheal tube/laryngeal mask placement, until extubation/removal or initiating transfer to a postoperative care location, shall be performed using a quantitative method such as capnography, capnometry or mass spectroscopy” (ASA, 2003).






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


