TOPICS
1. The clinical signs and symptoms of MV diseases
2. Physiologic compensatory mechanisms of MV diseases
3. Echocardiography and MV diseases
4. Surgical and catheter-mediated approaches to the repair/replacement of the MV.
5. Surgical approaches to the management of atrial fibrillation
6. Anesthetic implications of MV diseases
While the aortic valve serves as the gateway to the systemic circulation, the mitral valve is a one-way door to the left ventricle (LV). When intact, the mitral valve makes sure that a stroke volume’s (SV) worth of blood is delivered to the LV. Should the valve be too tight as in mitral stenosis (MS), the LV is underloaded reducing the SV (Video 7–1A-C). Moreover, the narrowed mitral valve prevents adequate drainage of the left atrium (LA) and the pulmonary circulation. With time, the LA dilates and pulmonary arterial (PA) pressures increase leading to the development of atrial fibrillation, pulmonary edema, and right ventricular failure. Consequently, these conditions make the anesthetic management of the MS patient for mitral valve (MV) replacement most challenging.
When the mitral valve becomes incompetent it no longer functions to ensure the one-way, forward flow of blood during each cardiac cycle. As the LV contracts during systole, blood can be ejected forward through the aortic valve (AV) into the systemic circulation, or the blood can flow retrograde into the LA via the leaky MV. Like aortic regurgitation (AR), mitral regurgitation (MR) can develop both acutely or exist chronically. Patients with chronic MR develop compensatory mechanisms, which permit them to eject a sufficient SV into the systemic circulation to maintain circulatory function. Conversely, the patient with acute MR lacks adequate compensatory mechanisms. Acute MR frequently presents secondary to papillary muscle dysfunction or rupture following myocardial infraction or due to the destruction of the valve during mechanical trauma or by infectious processes. As such, the acute MR patient usually presents in cardiogenic shock as the SV ejected into the systemic circulation is inadequate to meet the patient’s metabolic demands.
THE CLINICAL SIGNS AND SYMPTOMS OF MV DISEASES
Mitral Stenosis
The normal area of the MV is 4 to 6 cm2. Isolated narrowing of the MV is frequently associated with rheumatic heart disease.1 MS is more likely to occur in female compared to male patients by a ratio of 2:1. Calcification of the MV independent of rheumatic heart disease occurs infrequently. However, MV calcification can occur in dialysis-dependent chronic renal failure patients. As the rheumatic process progresses the valve area declines leading to an increased pressure gradient between the LA and the LV during diastole. This increased gradient drives diastolic filling of the LV as blood is pushed forcefully through the stenotic MV orifice.
As the gradient progressively increases and mitral valve area falls below 1.5 cm2, patients become increasingly symptomatic. Pressure gradients between the LA and LV can become greater than 25 mm Hg. Patients frequently become dyspneic as the high LA pressure is transmitted to the pulmonary vasculature. Pulmonary arterial pressures increase at times leading to pulmonary edema. Patients with MS may be asymptomatic at rest but when diastolic time is decreased (such as during exercise, stress, or pregnancy) the LA may not have sufficient time to empty and to load the LV—reducing the SV and increasing LA pressure. Increased LA pressure is transmitted to the pulmonary vasculature and the patient becomes dyspneic. Likewise, as the LA becomes distended secondary to MS, the patient can develop atrial fibrillation. Atrial fibrillation, especially when accompanied by rapid ventricular rate, reduces diastolic filling time, which in conjunction with the lack of atrial contraction at the end of diastole, further decreases LV filling and increases LA pressure leading to the patient becoming even more symptomatic.
Chronic Mitral Regurgitation
Many disease processes can acutely or chronically disrupt the integrity of the MV apparatus. For the valve not to leak, the valve annulus, leaflets, chordae, and papillary muscles must function properly (Video 7–2). Should the heart dilate secondary to cardiomyopathy the annulus can become enlarged preventing the coaptation of the anterior and posterior valve leaflets during systole—resulting in regurgitation (Figure 7–1 and Video 7–3). Should the papillary muscles or chordae be dysfunctional, torn, or stretched, the leaflets can prolapse or flail into the LA during systole—again resulting in regurgitation (Figure 7–2 and Videos 7–4A and B). Similarly, should a leaflet be too short or restricted, it will not be able to effectively close during systole (Figure 7–3 and Video 7–5). Finally, any disease process, which destroys or damages the leaflets, will also cause the regurgitation of blood into the LA during ventricular systole.
Various diseases including coronary artery disease, cardiomyopathies, rheumatic heart disease can lead to chronic MR. Patients can tolerate mild to moderate chronic MR for many years until they become increasingly dyspneic with exertion. As chronic MR is often secondary to other cardiac diseases such as coronary artery disease, it is difficult to differentiate between the symptoms of the chronic MR and those of the underlying cardiac disease.
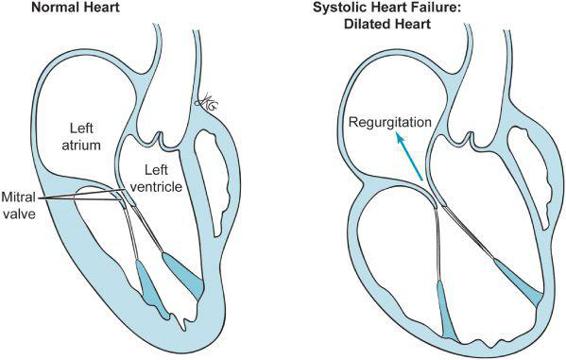
Figure 7–1. Dilatation of the heart results in the leaflets of the mitral valve failing to coapt resulting in central mitral regurgitation.
Acute Mitral Regurgitation
Acute MR occurs when the mitral apparatus becomes acutely dysfunctional. Patients may present in shock in the setting of an acute myocardial infarction with papillary muscle ischemia. Similarly, endocarditis can lead to loss of MV integrity resulting in acute MR and cardiogenic shock (Video 7–6). Patients are often dyspneic and in congestive heart failure. Such cases usually require emergent surgery if they are to be salvaged. Intra-aortic balloon pump (IABP) placement may be temporarily needed to reduce LV afterload so to minimize regurgitation until surgery can be commenced.
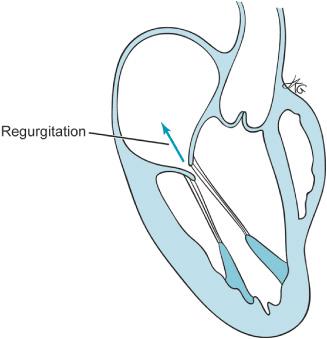
Figure 7–2. Mitral regurgitation can also occur when there is too much motion of the leaflets of the mitral valve as depicted here. The anterior leaflet of the mitral valve has too much movement compared to the posterior leaflet resulting in failure to coapt and mitral regurgitation.
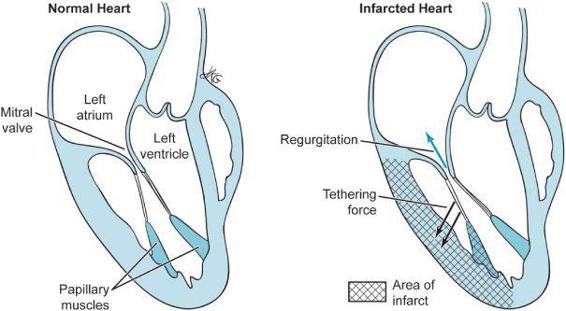
Figure 7–3. Mitral regurgitation also occurs where the movement of a mitral valve is restricted such as can occur following myocardial infarction.
PHYSIOLOGIC COMPENSATORY MECHANISMS OF MV DISEASES
The heart of the patient with MV disease attempts to compensate for the inability of the MV to ensure efficacious loading of the LV and ejection of an adequate SV into the systemic circulation. The LV of the patient with MS is chronically underloaded while that of the patient with MR is either acutely or chronically volume overloaded.
MR can occur either from a primary defect in the structure of the MV or secondary to abnormalities in the structure or geometry of the LV. As the LV dilates secondary to cardiomyopathy or ischemia, the papillary muscles shift caudally to the valve and can prevent the leaflets from effectively closing. Moreover, annular dilatation is also contributory.
The heart of the MR patient must respond to the increased volume load presented to it during each diastolic filling period.2–5 In the patient with an incompetent MV, during ventricular systole the SV is not fully ejected out through the AV into the systemic circulation. Rather, a good percentage of the SV enters the LA. To compensate, the LV hypertrophies eccentrically and dilates allowing for a greater left ventricular end-diastolic volume (LVEDV). This dilatation can further worsen MR. Concurrently, the LA dilates to accommodate the regurgitant volume. The increase in LVEDV is often accomplished without an increase in left ventricular end-diastolic pressure (LVEDP). Consequently, patients can tolerate chronic MR for many years because they maintain the forward SV by increasing the size of the LV.
Unfortunately, as with all of these compensatory mechanisms there are limits to their ability to maintain near-normal physiologic function in the setting of abnormal structural function. As the disease progresses, the heart increasingly dilates and contractile function deteriorates. LV compliance becomes decreased, thereby reducing the ability of the heart to accommodate increased LVEDV with only minimal changes in LVEDP. Additionally, ventricular remodeling increases the ratio of ventricular radius to ventricular wall thickness.4 This increased ratio together with an increase in LVEDP will result in an increase in wall stress according to the LaPlace law:
LV wall stress = (LV pressure × LV radius)/LV thickness
This increase in wall stress ultimately leads to an increase in myocardial oxygen demand.
The increased LVEDP is transmitted to the left atrium raising the left atrial pressure (LAP). Patients become progressively dyspneic and fatigued, as the heart can no longer eject a near normal SV into the systemic circulation.
The patient with acute MR does not have time to develop compensatory mechanisms for the reduction in forward flowing SV. When the MV becomes acutely incompetent, a part of the total SV is ejected in a retrograde manner in to the LA during systole.
Total SV = Forward Flowing SV + Retrograde Flowing SV
In the chronic MR patient, the total SV is increased secondary to dilation of the LV to compensate for that part of the total SV, which flows retrograde (retrograde flowing SV). Consequently, the forward flowing SV remains largely unchanged until the compensatory mechanisms are overwhelmed and the heart fails.
The patient with acute MR cannot increase the total SV since there is no time for such compensatory mechanisms to develop. Therefore, the forward flowing SV is reduced. The patient often presents in cardiogenic shock secondary to a reduced forward cardiac output. Concurrently, the LA cannot accommodate the regurgitant volume resulting in increased pulmonary pressures and pulmonary congestion.
The heart of the patient with MS must compensate for the chronic underloading of the LV and a reduced SV. Additionally, the pulmonary vasculature must mitigate the effects of increased LAP to prevent pulmonary congestion.
In patients with MS, a pressure gradient develops between the LA and LV during diastole. Recall, the SV is loaded into the LV during diastole. The stenotic MV impedes the delivery of blood to the LV. As the MV area decreases an increased LAP develops as blood is forced to flow through the narrowed MV orifice. This increased LAP is transmitted to the pulmonary veins. Should atrial fibrillation develop or the patient become tachycardic for any reason the patient will have a decrease in diastolic time—further reducing the time that the SV can pass through the narrowed orifice of the MV into the LV. Left atrial pressure further increases leading to pulmonary congestion. At the same time, the SV is progressively reduced as the LV is inadequately loaded. Patients become increasingly inactive, as the SV cannot meet the needs of the patient to conduct normal life activities.
The pulmonary vasculature tries to mitigate the increase in LAP in order to protect against the development of pulmonary edema. Pulmonary arteriolar changes may protect the pulmonary capillary bed by making it less leaky in the setting of high pulmonary venous pressures.1 Although such compensatory mechanisms may retard the development of pulmonary edema, they produce over time profound pulmonary hypertension (Chapter 8). Increasing resistance in the pulmonary arteries requires the right ventricle (RV) to do increased pressure work to pump the SV through the pulmonary vasculature. Although the RV responds with compensatory mechanisms to this pressure challenge, in time, RV failure ensues leading to peripheral edema, ascites, and hepatic failure. Consequently, the compensatory responses of the heart and pulmonary vasculature to MS can produce profound pulmonary hypertension and RV failure. Additionally, the chronically underloaded LV may itself have impaired contractility. Following relief of MS, the patient’s chronically underloaded LV may not be able to accommodate the additional volume load presented to it in diastole through an open mitral valve without becoming distended with a very high LVEDP.
ECHOCARDIOGRAPHY AND MV DISEASES
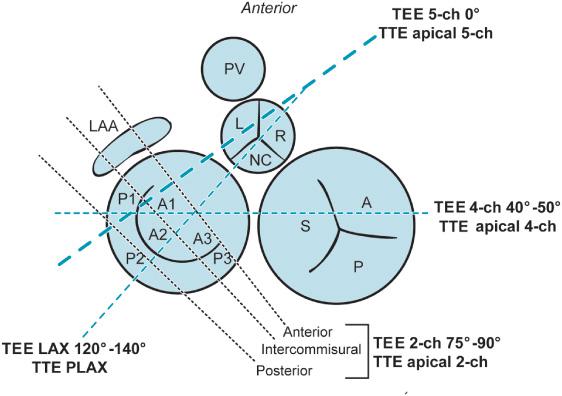
Transthoracic echocardiography (TTE) is an initial step in the cardiologist’s diagnosis of the MV patient. Perioperatively TEE is most likely to be employed to assist the surgeon performing MV repair or replacement.6 Three-dimensional TEE is becoming more commonly available and is used increasingly to examine the mitral valve perioperatively (Video 7–7). The basic TEE views of the normal mitral valve were discussed in the introduction to echocardiography and should be briefly reviewed before proceeding with this section (Figure 7–4).
Mitral Stenosis
The anterior and posterior leaflets of the MV appear thickened and poorly mobile in patients with mitral stenosis. As the patient’s valve becomes stenotic, the orifice narrows obstructing diastolic filling of the LV.
When performing a perioperative TEE examination in the MS patient it is also critical to look for additional echo findings associated with mitral stenosis such as a dilated left atrium with stagnant blood (Video 7–8). The smoky appearance or spontaneous echo contrast is indicative of decreased blood velocities in the LA. The two-chamber view demonstrates both the MV and the beak-like left atrial appendage (LAA). The LAA is often the site of clot formation; the clot can be removed at the time of surgery and the LAA subsequently ligated. Left and right ventricular function is often impaired in the MS patient secondary to LV underloading, pulmonary hypertension, and RV failure.
Cardiologists employ both TTE and TEE to examine and quantify the mitral valve.7,8 Perioperatively the valve area and pressure gradient across the MV will have already been determined before the patient is referred for surgery. Nonetheless, it is important to be able to assess the pressure gradient and estimate valve area in the operating room. Doppler measurements and the Bernoulli equation are used perioperatively to determine the transmitral pressure gradient between the LV and the LA.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


